Max has, over the past few weeks, really increased his ability to prop himself up on his forearms and control his head while doing so. He still can't hold the position for more than a few seconds, but that's a lot better than even a few weeks ago. Here are a couple of pictures of Max doing a half push-up:

Carolyn likes this one because it looks like he's riding a bucking bronco
Here Max is pushing himself up:

And here is a picture of Max collapsed on his face after the exertion.

Resting up for the next struggle
In these cycles of pushing up and collapsing, Max never gives up. He'll lie on his face and gather strength for another attempt, even if he needs more and more time to rest.
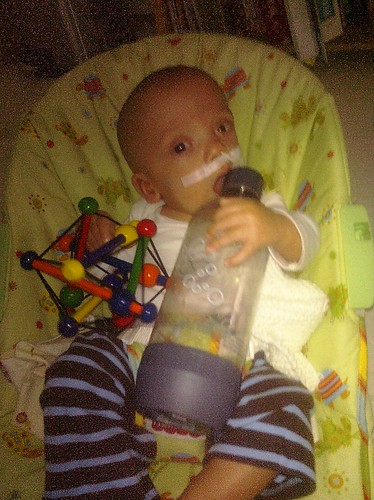
Max's fine motor skills have also improved. Here he's holding a bottle. He won't do anything useful with it, like sucking it dry, but he can handle it pretty well.

This is a fun toy--what am I supposed to do with it again?
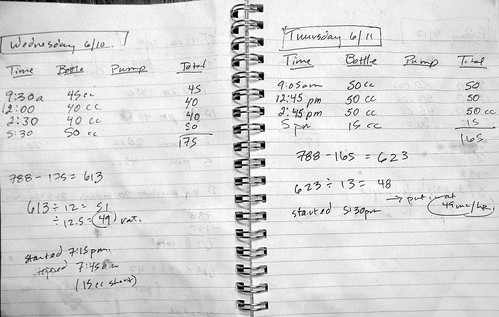
Even though he's only taking 130 to 150 ccs by mouth per day (against a total daily intake of 800 ccs), his oral competence remains good. He doesn't drool. Well, not more than most babies, I suppose. And he's fearless about putting things into his mouth. He's taken to sucking on his thumb:

It's like a pacifier that I always have with me
And when he encounters something new, his first instinct is to gnaw on it:

Speaking of toys Max always has with him, he's always been fascinated by his own feet. He can now grab them, and gets endless pleasure in catching them. The mystery still hasn't worn off:

Max started on his back, grabbed his feet and slowly toppled over
Unlike his older brother, Max enjoys pressure against his legs and feet. Where Felix treated the floor like it was hot lava, Max doesn't jerk his legs up when he's lowered onto the ground. He wants to stand:

All of this physical therapy and exertion mean that Max's arms and legs are much stronger than Felix's were at the same age. But Felix had much better control of his body, especially his head. This, in a nutshell, is the problem of "tone". That is, the problem Max's brain has in communicating with his muscles. His brain is shouting at his floppy neck and chest to support his head; Max's arms and legs are getting the message loud clear, but can't help much with controlling his head. But with all the demands for action from the brain, the arms and legs have to see some action.
On the crucial issue of Max's head control, we have seen some improvement. As we expected, it's a gradual process with only incremental progress. And, again, as we expected, there have been plenty of setbacks. What didn't I expect? I have been completely surprised by Max's tenacity combined with his unfailing good humor. Max will spend as long as it takes for him to push himself up enough to get a short glimpse over his crib bumpers. When his arms give out he lies on his stomach; he doesn't cry during any of this. He just gathers his strength for the next time he will push himself enough to see the wider world without anyone's help.















{kind=link}
{kind=link}
{kind=link}