Carolyn went into the NICU this morning having heard that Max had some dark vomit on his clothing very early this morning. It was the vitamins again! Perhaps Carolyn is on to something with her suspicions.
But the big news today was that nurse J. suggested Carolyn unplug Max from his monitors and take him for a walk. Max clearly enjoyed it; he stared at the pictures on the wall, he turned to voices when people to spoke to him, and made the soft cooing noises we sometimes hear from him when he's particularly content. Carolyn even took Max out into the waiting area between the two nurseries (the step-down nursery remains closed for lack of business). When Carolyn walked Max around, the standard rules of the NICU were all suspended, including the first rule of the NICU, which is not to talk to the other parents. Carolyn had a pleasant chat with the only other parents that have been there as long as we have. Because of the complete lack of privacy in the NICU we can't avoid following their child's progress; nor have they been able to avoid following Max's. It was nice, for a few minutes at least, to admire each others' babies, like real parents.
Carolyn is also quietly polling the nurses for their opinion of whether Max should have surgery to attempt to correct his reflux. Nurse J. reminded Carolyn that Max has had severe reflux almost since the start, certainly since mid-December, and he's had several opportunities to overcome it. She also said that in her experience she seen only very few complications from the surgery.
As for Max's reflux today, I would grade his progress as only fair. He spit up a couple of times, but not very much, and once because of the accursed vitamins. He had a very smooth feeding in the early afternoon, but his 5:00 PM feed was tough, with Max showing obvious signs of discomfort.
Finally, the nurses and Carolyn managed to get Max to take his Maalox by mouth. This is a milestone in my opinion, because taking food by mouth is something Max failed spectacularly at his first attempt back in December. At the time, the NICU team pointed out that the mechanics of swallowing depend critically on having a functioning and organized brain, and they blamed Max's problems on his hydrocephalus. Getting Max to swallow his Maalox wasn't easy: they had to put the Maalox in his mouth and then get him interested in his pacifier. A few sucks, a swallow, and it was down.
Saturday, January 31, 2009
The immediate future
Carolyn and I are still digesting the huge bolus of information we got at yesterday's two-hour family meeting. Certain topics we've simply decided not to obsess about until we can sit down with a specialist for more analysis.
Max's reflux, and potential surgery to correct it, are on the front burner. Essentially, Max is in the hospital now just because of his reflux. It requires that his feeds be stretched out over lengthy periods, it's inflaming his esophagus, and it's stressing his lung out because he often inhales the aspirated milk. Over the next few days the NICU team are going to try to form a picture of Max's esophagus and stomach using x-rays, barium studies and the like. This will help them plan for his surgery. At the same time, they're giving him one last chance to control the reflux on his own. It's Max's latest race against time (the head shunt and biopsy for Hirschsprung's being the most recent). Max has proved the NICU team wrong time and again, so Carolyn and I continue to hope--with some justification--that Max will avoid surgery next week.
There are good reasons to consider the surgery. But I also suspect that, perhaps unconsciously, the NICU team are looking for any kind of solution, and thus the surgery presents a kind of logical action for them. Without the surgery, I think that they may be at the end of their playbook. Beyond this, there is nothing but continued hospitalization and incremental progress. I'm reminded of Cavafy's poem about Rome on the day the barbarians were supposed to sack it. The barbarians don't, after all, appear that day and Rome's citizens are far from happy. The last line of the poem reads: And now, what's going to happen to us without barbarians?/ They were, those people, a kind of solution.
That said, I can imagine life with Max at home post-surgery. He'll have a g-tube (a direct tube to his stomach from the outside) through which we will feed him. He'll have frequent visits to doctors and to therapists. And no doubt he'll be one fussy infant. I mean, wouldn't you be too? He will be within his rights under the Baby Geneva Conventions to wake us up every two hours and to vomit on all available surfaces. But he'll also be a baby at home with his parents. He will do all those things that babies do that we forget about (because sleep deprivation inhibits memory formation). Why do we only remember the bad things? The other things are fun, and fun is good.
Max's reflux, and potential surgery to correct it, are on the front burner. Essentially, Max is in the hospital now just because of his reflux. It requires that his feeds be stretched out over lengthy periods, it's inflaming his esophagus, and it's stressing his lung out because he often inhales the aspirated milk. Over the next few days the NICU team are going to try to form a picture of Max's esophagus and stomach using x-rays, barium studies and the like. This will help them plan for his surgery. At the same time, they're giving him one last chance to control the reflux on his own. It's Max's latest race against time (the head shunt and biopsy for Hirschsprung's being the most recent). Max has proved the NICU team wrong time and again, so Carolyn and I continue to hope--with some justification--that Max will avoid surgery next week.
There are good reasons to consider the surgery. But I also suspect that, perhaps unconsciously, the NICU team are looking for any kind of solution, and thus the surgery presents a kind of logical action for them. Without the surgery, I think that they may be at the end of their playbook. Beyond this, there is nothing but continued hospitalization and incremental progress. I'm reminded of Cavafy's poem about Rome on the day the barbarians were supposed to sack it. The barbarians don't, after all, appear that day and Rome's citizens are far from happy. The last line of the poem reads: And now, what's going to happen to us without barbarians?/ They were, those people, a kind of solution.
That said, I can imagine life with Max at home post-surgery. He'll have a g-tube (a direct tube to his stomach from the outside) through which we will feed him. He'll have frequent visits to doctors and to therapists. And no doubt he'll be one fussy infant. I mean, wouldn't you be too? He will be within his rights under the Baby Geneva Conventions to wake us up every two hours and to vomit on all available surfaces. But he'll also be a baby at home with his parents. He will do all those things that babies do that we forget about (because sleep deprivation inhibits memory formation). Why do we only remember the bad things? The other things are fun, and fun is good.
Friday, January 30, 2009
Max's monitor
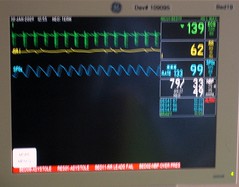
I've been meaning to post a picture of Max's NICU monitor for quite a while. It turns out to be really hard to take a picture of a computer monitor, so I apologize for the blurriness.
The monitor tracks heart rate, respiratory rate, measured oxygen saturation and blood pressure. There's also a list of the most recent alarms. For example, one alarm line reads "DESAT 87 12:37". Max's measured oxygen saturation fell to 87 percent (below the alarm threshold of 88 percent) at 12:37. With Max's reflux increasing in severity, his desat alarms are again becoming more common. Back when his feeding tube was in his duodenum, Max almost never had a desat.
We'll bring Max home with a lower-tech version of this monitor, one that doesn't report values. I'm told it merely emits a piercing wail when one of the measures strays out of bounds.
The monitor tracks heart rate, respiratory rate, measured oxygen saturation and blood pressure. There's also a list of the most recent alarms. For example, one alarm line reads "DESAT 87 12:37". Max's measured oxygen saturation fell to 87 percent (below the alarm threshold of 88 percent) at 12:37. With Max's reflux increasing in severity, his desat alarms are again becoming more common. Back when his feeding tube was in his duodenum, Max almost never had a desat.
We'll bring Max home with a lower-tech version of this monitor, one that doesn't report values. I'm told it merely emits a piercing wail when one of the measures strays out of bounds.
Another big family meeting
We had a "family meeting" today; our first in two months. Max's entire NICU team assembled in a conference room adjacent to the critical care nursery: the attending, fellow, resident, Max's nurse and a social worker, plus maybe a couple other cast members took two hours out of their day to talk to us and answer our questions. I feel like writing a personal note of apology to all of the babies in the NICU because we sucked up so much of the NICU team's collective brainpower.
We learnt quite a bit: too much for me to detail tonight. I will hit the high points now and then write a longer description later. (If you stick around to the end of this post you'll be rewarded with a heart-warming story.) The attending began the discussion of each of Max's problems by asking us to describe our perception of the situation. The picture that Carolyn and I described seemed to accord well with the NICU team's in almost all cases, so there weren't (many) surprises.
I'll start with Max's head because I believe that, although it is not an urgent problem right now, many years from now we'll still be dealing with Max's hydrocephalus long after we've forgotten about his reflux or breathing problems. Thus, any kind of news about his hydrocephalus affects my vision of life in the science-fictional year of 2030 (when I hope to attend Max's college graduation). As we knew, Max has hydrocephalus, but his most recent MRI showed no sign of PVL. However, Dr. S. said that in addition to being swollen (the hallmark of hydrocephalus), Max's left ventricle was oddly shaped. I think that Dr. S. adduced that the ventricle may have flowed into an area of "lost brain". As I understand it, until now we'd been worried about the damage that Max's ventricles did to the surrounding brain tissue when they filled with CSF and expanded. However, Dr. S. seemed to suggest that, like a water balloon sitting on some Legos, one of Max's ventricles might be larger than normal because there was no brain tissue there to push back. This was all very confusing, and we asked several questions about it but couldn't quite nail down what had happened. Carolyn and I have decided to suspend our anxiety on this matter and consult with a neurologist next week. We also learnt that 20 percent of infants with enlarged ventricles go on to have some kind of motor or cognitive deficit.
We can't control what's going on inside Max's brain. However, I'm firmly convinced that aggressive therapy can ameliorate any damage. Dr. S. and the NICU team clearly relaxed when we said that we intended to sign Max up for the local early intervention program and follow the advice of speech/physical/occupational therapists. Years of graduate school have prepared Carolyn and me to compulsively follow any therapeutic regimen suggested by the experts. I also told the NICU team what they couldn't know: that Max's older brother is as sharp as a tack, and that his parents aren't dullards either. Hence, Max himself must be in line to inherit some grade A brains. This was the one comment I made that elicited hearty laughter from the whole NICU team. Perhaps Max's dad isn't as smart as he thought.
The NICU team told us that a recent assessment of Max's reflexes, behavior, etc put him at the same level as a normal baby aged one month. (Max is more than three months old.) I think the NICU team were afraid that this would dismay us, but Carolyn and I were thrilled by the news. Considering that for weeks and weeks of his early tenure at the NICU, Max wasn't even as responsive as a normal newborn infant, this is a huge step forward.
Dr. S. was quite upbeat about the state of Max's lungs. First, the bad news: the lungs were damaged by the use of oxygen therapy and respirators in his early weeks at the NICU, plus the normal underdevelopment of the lung of the premature infant. In addition, Max is aspirating his reflux (see below) further damaging them. The inflammation from inhaling liquids is what is causing his persistent pulmonary edema, which decreases the efficiency of his lungs.
Now the good news. The lung seems to be the one organ that NICU teams really love. It grows relatively quickly in relation to the infant's overall growth, and grows for a long time. By the time Max is two years old, the damaged portion of his lung will represent only a small fraction of his overall lung. Even if Max's reflux continues to damage his lung, it will grow its way out of trouble. The danger to Max's lung is that he aspirates a considerable quantity of milk and develops pneumonia: this could affect a significant fraction of his lung.
Finally, we spent quite a lot of time talking about Max's main problem: his reflux. Really, his reflux is the main reason Max is still in the hospital. I think they would have sent him home with a feeding tube by now. But when Max is fed he is very uncomfortable and is clearly feeling his stomach contents travelling up his esophagus. He vomits much more frequently now than ever before in his stay at the NICU. To Carolyn and me this reflux seemed to come out of nowhere. However, the NICU team told us that they've increased the volume that Max is getting. This is actually good news: despite his reflux and vomiting, Max is managing to get enough nutrition from his feeds that he is gaining weight. Indeed, in a very narrow sense, I believe that Max is actually maybe thriving. Some babies require supplemental nutrition via an IV. In addition, back during the dark days of mid-December, I remember Max's nurses describing his symptoms as consistent with reflux. Shortly after that, the NICU team pushed his feeding tube into his duodenum, where it was more or less impossible for milk to return to the stomach and then reflux back to the esophagus.
The NICU team are urging us to seriously consider a couple of linked surgical procedures. First is running a tube--called a g-tube--to Max's stomach directly from the outside world. This will allow us to feed him without using a feeding tube. If Max didn't have reflux but was just having trouble eating, a g-tube would allow us to take him home immediately. The second is called the Nissen procedure and involves, effectively, tightening the esophagus's opening into the stomach. This surgery elicits a lot of controversy on the Internet. Many parents seem to feel that their doctors suggest it as a way to get a baby to stop screaming in discomfort from reflux, but that the procedure itself doesn't actually do much. In adults, the procedure isn't that successful.
The good news is that the NICU team are very conservative and will consult closely with the pediatric surgeon. They're ordering a couple of barium studies of his esophagus to see whether there's a structural abnormality that might make Max a good candidate for a Nissen. We've gotten to know the surgeon quite well over the past few months because Max has come close to requiring his services at least twice. We like and trust him. He wasn't the least bit disappointed in the past episodes when Max got himself organized and avoided the surgeon's knife.
And now, the heart-warming story. Carolyn went out for coffee with a colleague this afternoon. When she returned, she found that Max's nurses had rigged up a system of pads to allow him to be slightly propped up but also comfortable. She had also set up a toy star with a little mirror on it just within Max's reach. Carolyn found Max happily reaching up and batting at the star. From her description, it seems like Carolyn spent some time just staring at the scene: a baby playing happily with a crib toy.
We learnt quite a bit: too much for me to detail tonight. I will hit the high points now and then write a longer description later. (If you stick around to the end of this post you'll be rewarded with a heart-warming story.) The attending began the discussion of each of Max's problems by asking us to describe our perception of the situation. The picture that Carolyn and I described seemed to accord well with the NICU team's in almost all cases, so there weren't (many) surprises.
I'll start with Max's head because I believe that, although it is not an urgent problem right now, many years from now we'll still be dealing with Max's hydrocephalus long after we've forgotten about his reflux or breathing problems. Thus, any kind of news about his hydrocephalus affects my vision of life in the science-fictional year of 2030 (when I hope to attend Max's college graduation). As we knew, Max has hydrocephalus, but his most recent MRI showed no sign of PVL. However, Dr. S. said that in addition to being swollen (the hallmark of hydrocephalus), Max's left ventricle was oddly shaped. I think that Dr. S. adduced that the ventricle may have flowed into an area of "lost brain". As I understand it, until now we'd been worried about the damage that Max's ventricles did to the surrounding brain tissue when they filled with CSF and expanded. However, Dr. S. seemed to suggest that, like a water balloon sitting on some Legos, one of Max's ventricles might be larger than normal because there was no brain tissue there to push back. This was all very confusing, and we asked several questions about it but couldn't quite nail down what had happened. Carolyn and I have decided to suspend our anxiety on this matter and consult with a neurologist next week. We also learnt that 20 percent of infants with enlarged ventricles go on to have some kind of motor or cognitive deficit.
We can't control what's going on inside Max's brain. However, I'm firmly convinced that aggressive therapy can ameliorate any damage. Dr. S. and the NICU team clearly relaxed when we said that we intended to sign Max up for the local early intervention program and follow the advice of speech/physical/occupational therapists. Years of graduate school have prepared Carolyn and me to compulsively follow any therapeutic regimen suggested by the experts. I also told the NICU team what they couldn't know: that Max's older brother is as sharp as a tack, and that his parents aren't dullards either. Hence, Max himself must be in line to inherit some grade A brains. This was the one comment I made that elicited hearty laughter from the whole NICU team. Perhaps Max's dad isn't as smart as he thought.
The NICU team told us that a recent assessment of Max's reflexes, behavior, etc put him at the same level as a normal baby aged one month. (Max is more than three months old.) I think the NICU team were afraid that this would dismay us, but Carolyn and I were thrilled by the news. Considering that for weeks and weeks of his early tenure at the NICU, Max wasn't even as responsive as a normal newborn infant, this is a huge step forward.
Dr. S. was quite upbeat about the state of Max's lungs. First, the bad news: the lungs were damaged by the use of oxygen therapy and respirators in his early weeks at the NICU, plus the normal underdevelopment of the lung of the premature infant. In addition, Max is aspirating his reflux (see below) further damaging them. The inflammation from inhaling liquids is what is causing his persistent pulmonary edema, which decreases the efficiency of his lungs.
Now the good news. The lung seems to be the one organ that NICU teams really love. It grows relatively quickly in relation to the infant's overall growth, and grows for a long time. By the time Max is two years old, the damaged portion of his lung will represent only a small fraction of his overall lung. Even if Max's reflux continues to damage his lung, it will grow its way out of trouble. The danger to Max's lung is that he aspirates a considerable quantity of milk and develops pneumonia: this could affect a significant fraction of his lung.
Finally, we spent quite a lot of time talking about Max's main problem: his reflux. Really, his reflux is the main reason Max is still in the hospital. I think they would have sent him home with a feeding tube by now. But when Max is fed he is very uncomfortable and is clearly feeling his stomach contents travelling up his esophagus. He vomits much more frequently now than ever before in his stay at the NICU. To Carolyn and me this reflux seemed to come out of nowhere. However, the NICU team told us that they've increased the volume that Max is getting. This is actually good news: despite his reflux and vomiting, Max is managing to get enough nutrition from his feeds that he is gaining weight. Indeed, in a very narrow sense, I believe that Max is actually maybe thriving. Some babies require supplemental nutrition via an IV. In addition, back during the dark days of mid-December, I remember Max's nurses describing his symptoms as consistent with reflux. Shortly after that, the NICU team pushed his feeding tube into his duodenum, where it was more or less impossible for milk to return to the stomach and then reflux back to the esophagus.
The NICU team are urging us to seriously consider a couple of linked surgical procedures. First is running a tube--called a g-tube--to Max's stomach directly from the outside world. This will allow us to feed him without using a feeding tube. If Max didn't have reflux but was just having trouble eating, a g-tube would allow us to take him home immediately. The second is called the Nissen procedure and involves, effectively, tightening the esophagus's opening into the stomach. This surgery elicits a lot of controversy on the Internet. Many parents seem to feel that their doctors suggest it as a way to get a baby to stop screaming in discomfort from reflux, but that the procedure itself doesn't actually do much. In adults, the procedure isn't that successful.
The good news is that the NICU team are very conservative and will consult closely with the pediatric surgeon. They're ordering a couple of barium studies of his esophagus to see whether there's a structural abnormality that might make Max a good candidate for a Nissen. We've gotten to know the surgeon quite well over the past few months because Max has come close to requiring his services at least twice. We like and trust him. He wasn't the least bit disappointed in the past episodes when Max got himself organized and avoided the surgeon's knife.
And now, the heart-warming story. Carolyn went out for coffee with a colleague this afternoon. When she returned, she found that Max's nurses had rigged up a system of pads to allow him to be slightly propped up but also comfortable. She had also set up a toy star with a little mirror on it just within Max's reach. Carolyn found Max happily reaching up and batting at the star. From her description, it seems like Carolyn spent some time just staring at the scene: a baby playing happily with a crib toy.
Thursday, January 29, 2009
Evening update (Thursday 1/29)
Max's day started at 8 a.m. sharp today with an exam by the neurologist who was looking at his tone, reflexes, etc. and who later would read his MRI. The doc said Max looked "good" but we don't yet know the official word. Next up, physical therapy with the rarely seen therapist C. We stopped his feed so that he could have physical therapy because he was awake and alert (physical therapy is less effective on a sleeping baby, although we still do it so as not to reward Max for his habit of "playing possum"). In hindsight mixing eating and exercise may have been a bad idea because he vomited up whatever had gone into his stomach just as C. was starting the PT routine. But after that he seemed fine and had a successful PT session, showing some headlifts, turning toward voices, reaching (ever so slightly) toward toys, and stretching, and kept good respiratory control throughout. After that exhausting morning, much of the rest of the day was spent snoozing (AND keeping his vitamins down) until about 5 p.m. when his eyes popped open.
The NICU team were unphased by Max's vomiting and bradys yesterday evening. They see this as just part of the process; they have come to share Andreas's crackpot view that Max is a "slow learner". After spreading his feeds over 2 hours throughout today, tonight they have compressed them back to 105 minutes. They also started Maalox to coat his stomach and esophagus with the goal of reducing pain from reflux.
In other news, the pediatric surgeon, Dr. C, stopped by for a preliminary eval in case Max needs a G-tube and fundoplication. This is the same doc who, a month or two ago, threatened Max with a rectal biopsy unless he had a bowel movement , after which Max did in fact decide to get his bowels moving. Dr. C had a very stern talk with Max at the bedside today (actually Dr. C is an incredibly kind person) and so maybe that will do the trick. Dr. C is not keen on rushing into surgery as long as Max seems to be making progress on the current course of treatment. He was going to recommend that some Xrays be taken today (which they were) to make sure there wasn't anything evident that was causing the recent daily vomiting and discomfort. Max will probably also have a barium study next week to look at his stomach, esophagus, etc. to see if there are any abnormalities.
Finally, Max took a road trip and moved back to the Big House (aka the primary NICU, not the step-down) late this afternoon, just before waking up. No changes in Max's condition. The staff were just consolidating the two units because business is slow (the NICU has a total of 15 patients). Max is back to his position by the window, and also by one of the nurses' stations where we hope he will get lots of attention. One of the nurses told me earlier this week that if she were 27 years younger, she would like to be Max's girlfriend.
The NICU team were unphased by Max's vomiting and bradys yesterday evening. They see this as just part of the process; they have come to share Andreas's crackpot view that Max is a "slow learner". After spreading his feeds over 2 hours throughout today, tonight they have compressed them back to 105 minutes. They also started Maalox to coat his stomach and esophagus with the goal of reducing pain from reflux.
In other news, the pediatric surgeon, Dr. C, stopped by for a preliminary eval in case Max needs a G-tube and fundoplication. This is the same doc who, a month or two ago, threatened Max with a rectal biopsy unless he had a bowel movement , after which Max did in fact decide to get his bowels moving. Dr. C had a very stern talk with Max at the bedside today (actually Dr. C is an incredibly kind person) and so maybe that will do the trick. Dr. C is not keen on rushing into surgery as long as Max seems to be making progress on the current course of treatment. He was going to recommend that some Xrays be taken today (which they were) to make sure there wasn't anything evident that was causing the recent daily vomiting and discomfort. Max will probably also have a barium study next week to look at his stomach, esophagus, etc. to see if there are any abnormalities.
Finally, Max took a road trip and moved back to the Big House (aka the primary NICU, not the step-down) late this afternoon, just before waking up. No changes in Max's condition. The staff were just consolidating the two units because business is slow (the NICU has a total of 15 patients). Max is back to his position by the window, and also by one of the nurses' stations where we hope he will get lots of attention. One of the nurses told me earlier this week that if she were 27 years younger, she would like to be Max's girlfriend.
Morning update (Thursday 1/29)
At the 2:00 AM call we learnt that the NICU team had decreased Max's feeding schedule to 120 minutes. Even before last night's double brady he was having trouble tolerating feeds over 90 minutes. This is a setback, and raises the chances in our mind that the NICU team are going to recommend a type of surgery to correct Max's reflux. This is a situation that Carolyn calls a race against time---will Max be able to regulate himself before the NICU team really insist on surgery? This has happened at least twice before, with his hydrocephalus and his intestinal defects. In those cases, he was able to figure out how to control his CSF system and his digestion before the surgeons were able to get to him. We're hoping for the same hair's-breadth escape this time.
Wednesday, January 28, 2009
Late night update (Wednesday 1/28)
At tonight's phone call check-in, nurse R. had some bad news. Max had two separate episodes of bradycardia and emesis, with associated desats. She wasn't sure he was tolerating the compression of feeds to 90 minutes very well.
Evening Update (Wednesday 1/28)
Max had another fair-to-middling day today. He spit up some in the morning (those darn vitamins again) and was clearly in pain from reflux at a late afternoon feed. One of the nurses has an infant at home with reflux and told Carolyn that her kid sometimes cries for three hours straight. And, of course, most babies spit up a little bit, hence the ubiquitous towel-over-the-shoulder look sported by parents everywhere. But it was still difficult to see Max in pain, and of course his breathing remains a little labored.
Speaking of which, Carolyn reports that Max's breathing was a little easier today than it was yesterday. He had some desats in the morning but none in the afternoon. While still pretty fast, his breathing was slower than yesterday and he retracted less severely. (Retracting is a characteristic movement of the chest that indicates the baby is working really hard to breathe.)
The audiologist tested Max's hearing: he passed, although like all preemies he'll have to be tested again in six months. The neurologist is dropping by for a routine evaluation tomorrow; he'll take his own look at the most recent MRI. And Carolyn and I are scheduled to have a "family meeting" with the attending, Dr. S., on Friday. Previous family meetings have been tense affairs, mainly because they took place in the midst of various crises. This family meeting promises to be less dramatic, more routine. We'll evaluate Max's progress along the path the NICU team laid out for him.
Overall, Carolyn and I are feeling some NICU fatigue. Maybe we became habituated to Max's early daredevil antics where he would teeter on the brink of some medical disaster (hydrocephalus! head bleeds! NEC!) and then gather strength for an amazing recovery. Thus, his current slow and halting progress is frustrating. The same kid who confounded the neurosurgeons just hours before they were going to crack his head open should be able to master eating and breathing in a snap. We'll find out more of the NICU team's opinion at the family meeting on Friday, but Max's progress feels to me like the slow end of normal for preemies; this is a huge improvement over the high-wire act of his early weeks, but, with many of those problems waning, it seems like time to bring him home.
We have his room all ready for him. Crib, soothing music, interesting mobile, coffee maker for mom and dad, it's all sitting around gathering dust. Max has come a long way since he was born, he's done a lot of work, all he has to do is take a few more steps and he'll have finished his part and he can let his parents start doing theirs.
Speaking of which, Carolyn reports that Max's breathing was a little easier today than it was yesterday. He had some desats in the morning but none in the afternoon. While still pretty fast, his breathing was slower than yesterday and he retracted less severely. (Retracting is a characteristic movement of the chest that indicates the baby is working really hard to breathe.)
The audiologist tested Max's hearing: he passed, although like all preemies he'll have to be tested again in six months. The neurologist is dropping by for a routine evaluation tomorrow; he'll take his own look at the most recent MRI. And Carolyn and I are scheduled to have a "family meeting" with the attending, Dr. S., on Friday. Previous family meetings have been tense affairs, mainly because they took place in the midst of various crises. This family meeting promises to be less dramatic, more routine. We'll evaluate Max's progress along the path the NICU team laid out for him.
Overall, Carolyn and I are feeling some NICU fatigue. Maybe we became habituated to Max's early daredevil antics where he would teeter on the brink of some medical disaster (hydrocephalus! head bleeds! NEC!) and then gather strength for an amazing recovery. Thus, his current slow and halting progress is frustrating. The same kid who confounded the neurosurgeons just hours before they were going to crack his head open should be able to master eating and breathing in a snap. We'll find out more of the NICU team's opinion at the family meeting on Friday, but Max's progress feels to me like the slow end of normal for preemies; this is a huge improvement over the high-wire act of his early weeks, but, with many of those problems waning, it seems like time to bring him home.
We have his room all ready for him. Crib, soothing music, interesting mobile, coffee maker for mom and dad, it's all sitting around gathering dust. Max has come a long way since he was born, he's done a lot of work, all he has to do is take a few more steps and he'll have finished his part and he can let his parents start doing theirs.
Tuesday, January 27, 2009
Late night update (Tuesday 1/27)
Nurse L. reports that Max had a little residual after his 5:30 PM feeding--which she put back into his stomach. He hasn't thrown up -- or had emesis to use medical jargon -- since his episode at 4:00 PM, and he tolerated his 8:30 PM feeding well. Nurse L. also told us that she thought Max needed some attention and picked him up and held him for a while. In all, a pretty positive report.
Evening Update (Tuesday 1/27)
An eventful day for Max in the NICU. The first feeding after Carolyn arrived--the 8:30 AM feeding--went smoothly. Max was asleep on his stomach at the time (a perk of the NICU--none of this "back to sleep" nonsense when you're wired up like Neal Armstrong). He got his vitamins--Carolyn's bête noire and usual explanation for Max's vomiting--in the 11:30 AM feeding. However, nurse N. went the extra mile and cleverly diluted the vitamins in his milk so that Max didn't get the normal concentrated dose of cheap tequila or whatever it is they make those vitamins out of. As a result, he tolerated them well.
Max started showing desats after he woke up during his 11:30 AM feeding. These may have been the result of a misplaced pulse oximeter, or they could have been signalling real respiratory distress. Nurse N. retaped the red light bulb that is used to measure his blood oxygen saturation and the frequency of his measured desats decreased. Real, or artifact of miscalibrated equipment? We'll never know.
However, throughout his 2:30 PM feed Max seemed quite uncomfortable. He was shifting position on Carolyn's lap frequently and complaining (in his baby way). Around 4:00 PM (i.e. at the end of his 90 minute feed) he puked up 20 to 30 ccs, out of the 70 ccs that they had fed him. After this he felt much better. However, he did have what looked a real desat at the same time.
Over the course of the day, Carolyn gave him a pass on his workout routine. (Nurse N.: You can't go to the gym every day. Amen sister.)
The good news--the news that makes up for his vomiting and desats--is that Carolyn and the nurses have been working with Max on his pacifier. He seems to have rediscovered the joys of using a pacifier. This is important for his oral competence and his plan to eventually break out of the NICU.
Max started showing desats after he woke up during his 11:30 AM feeding. These may have been the result of a misplaced pulse oximeter, or they could have been signalling real respiratory distress. Nurse N. retaped the red light bulb that is used to measure his blood oxygen saturation and the frequency of his measured desats decreased. Real, or artifact of miscalibrated equipment? We'll never know.
However, throughout his 2:30 PM feed Max seemed quite uncomfortable. He was shifting position on Carolyn's lap frequently and complaining (in his baby way). Around 4:00 PM (i.e. at the end of his 90 minute feed) he puked up 20 to 30 ccs, out of the 70 ccs that they had fed him. After this he felt much better. However, he did have what looked a real desat at the same time.
Over the course of the day, Carolyn gave him a pass on his workout routine. (Nurse N.: You can't go to the gym every day. Amen sister.)
The good news--the news that makes up for his vomiting and desats--is that Carolyn and the nurses have been working with Max on his pacifier. He seems to have rediscovered the joys of using a pacifier. This is important for his oral competence and his plan to eventually break out of the NICU.
Monday, January 26, 2009
Evening update (Monday 1/26)
Max greeted Carolyn this morning by throwing up a large portion of his morning feed. (Carolyn as usual blames Max's morning vitamin dose.) Max held down the rest of his feeds today, although Carolyn reports that he sometimes got a strange, inward-looking expression on his face as if though he were considering vomiting, but he never again did. So it was a close-run thing in a couple of cases. He was bright-eyed and alert for most of the day. His breathing continues to be good, with few or no desats.
Yesterday, Carolyn was worried because he seemed to be slacking off on his pacifier use, a potential sign of diminished oral competence which will cause trouble down the road when he learns to eat by mouth and, of course, when he tries to talk. Today, she got him to take his pacifier after several rejections. Max, like many babies, has trouble keeping his pacifier in even when he wants to suck on it. Carolyn propped Max up against his stuffed elephant in an arrangement where the elephant's trunk held the pacifier in.
Tonight's nurse, J., is our kind of person. She is working with Max on his pacifier (when he's awake). She noticed that he was up and fussy earlier this evening and decided to give him a bath and massage. This quieted him down. Nurse J. believes that the day is a time for fun and stimulation, but that the night is a time for sleeping.
Max crossed another threshold tonight: his weight, at 4,085 grams, is now just a hair over 9 lbs.
I'm pasting in a picture of the helpful elephant below. Note that it was hand-knit --- an accomplishment in differential geometry.

Yesterday, Carolyn was worried because he seemed to be slacking off on his pacifier use, a potential sign of diminished oral competence which will cause trouble down the road when he learns to eat by mouth and, of course, when he tries to talk. Today, she got him to take his pacifier after several rejections. Max, like many babies, has trouble keeping his pacifier in even when he wants to suck on it. Carolyn propped Max up against his stuffed elephant in an arrangement where the elephant's trunk held the pacifier in.
Tonight's nurse, J., is our kind of person. She is working with Max on his pacifier (when he's awake). She noticed that he was up and fussy earlier this evening and decided to give him a bath and massage. This quieted him down. Nurse J. believes that the day is a time for fun and stimulation, but that the night is a time for sleeping.
Max crossed another threshold tonight: his weight, at 4,085 grams, is now just a hair over 9 lbs.
I'm pasting in a picture of the helpful elephant below. Note that it was hand-knit --- an accomplishment in differential geometry.
Sunday, January 25, 2009
Evening Update (Sunday 1/25)
With the sainted Dr. B. now replaced by the more minatory Dr. K. the NICU feels a little more dangerous. However, so far Max continues to make progress. The NICU team compressed his feeds to 90 minutes this morning. He spit up a little of his first feeding at this new speed, although Carolyn feels that the foul-smelling vitamins he was also given played a role. If you'd smelled them, you would have vomited too is her view. The NICU team have also put Max's reglan "on hold" because his stools were somewhat runny.
Carolyn gave Max a mani/pedi (the NICU team don't clip toenails/fingernail as a rule). She observed--and a couple of nurses have also reported--that Max doesn't that interested in his pacifier any more. Something to work on with the speech therapists. Carolyn also reports that Max was pretty drowsy all day. Max and Carolyn did however read The Very Hungry Caterpillar, and Max enjoyed the last page, where the caterpillar wakes up as a butterfly.
Carolyn gave Max a mani/pedi (the NICU team don't clip toenails/fingernail as a rule). She observed--and a couple of nurses have also reported--that Max doesn't that interested in his pacifier any more. Something to work on with the speech therapists. Carolyn also reports that Max was pretty drowsy all day. Max and Carolyn did however read The Very Hungry Caterpillar, and Max enjoyed the last page, where the caterpillar wakes up as a butterfly.
Saturday, January 24, 2009
Evening update (Saturday 1/24)
Max enjoyed another quiet day and night. Max continues to tolerate his feeds; he's still getting his feeding over 105 minutes, but the NICU have increased the volume that they're feeding him. He is after all more than eight pounds now. Max held Carolyn at the NICU this evening by slyly pulling off all of his leads just as she was leaving, and also demanding a fresh diaper.
Carolyn tells me that since Max's MRI showed no PVL the doctors and nurses seem to have a different attitude towards him. Perhaps it's merely our perception, but it seems that the NICU team now see that Max could grow up into a normal healthy boy (something we never doubted).
Carolyn tells me that since Max's MRI showed no PVL the doctors and nurses seem to have a different attitude towards him. Perhaps it's merely our perception, but it seems that the NICU team now see that Max could grow up into a normal healthy boy (something we never doubted).
Friday, January 23, 2009
Evening Update (Friday 1/23)
A quiet day for Max. Nurse N. printed out the official radiologist's report from the MRI the NICU team ordered on January 21. The last sentence read something like "No evidence of PVL". We'd already gotten the unofficial word that the doctors hadn't seen any damage in the MRI, but until we got the official report from the radiologists, we were slightly on edge.
Max continued to get his feeds over 105 minutes. He did extremely well, with one notable exception. Towards the end of one of his feeds, he visibly struggled with some reflux and then had a brady and desat. It was all over quickly, and the NICU team didn't have to hit him with supplemental oxygen or extra stimulation. This is the first brady he's had in weeks. But I can remember the days when I was routinely rubbing his chest or back trying to get his heart rate back up.
Today was the sainted Dr. B.'s last day on her rotation as the "attending" or chief doctor of the NICU. As a good public manager, Carolyn looked Dr. B. in the eye and thanked her for a specific set of achievements (management rule #1: "when you see it, say it"). I thought perhaps that after her rotation in charge of Max's care, Dr. B. might enjoy being Surgeon General. My brother pointed out that President Obama long ago nominated someone from television to be Surgeon General. Well, maybe Dr. B.'s chance will come next term.
Max continued to get his feeds over 105 minutes. He did extremely well, with one notable exception. Towards the end of one of his feeds, he visibly struggled with some reflux and then had a brady and desat. It was all over quickly, and the NICU team didn't have to hit him with supplemental oxygen or extra stimulation. This is the first brady he's had in weeks. But I can remember the days when I was routinely rubbing his chest or back trying to get his heart rate back up.
Today was the sainted Dr. B.'s last day on her rotation as the "attending" or chief doctor of the NICU. As a good public manager, Carolyn looked Dr. B. in the eye and thanked her for a specific set of achievements (management rule #1: "when you see it, say it"). I thought perhaps that after her rotation in charge of Max's care, Dr. B. might enjoy being Surgeon General. My brother pointed out that President Obama long ago nominated someone from television to be Surgeon General. Well, maybe Dr. B.'s chance will come next term.
Thursday, January 22, 2009
Evening Update (Thursday 1/22)
Today Max and I held hands, cuddled, sang the ABC song and other favorites, did some stretches, and napped. Max continues to tolerate his feeds (now over 105 minutes) well - no desats, bradys, tachypnea etc. While he still sounds snuffly and clearly is battling reflux, so far it does not seem to be affecting his lungs. He had a good day, perhaps buoyed by his great MRI news. The nurses and docs commented about how good and "pink" he looked, almost as if he had been transfused with more blood (he hasn't been). For those of you who miss the play-by-play on Max's stooling behaviors, you will be happy to know that he had a big day of big diapers and gas passing. The nurses could hear him from across the room and he was really stinking up the joint. Nurse L., who is taking care of Max tonight, said that he was awake this evening and looking around for stimulation from toys, nurses, anyone/thing who would give him the time of day. (Dr. B. also told me that Max seemed to notice her as she walked by yesterday, which was a big hit.) We are looking forward to having Max come home so he can get all kinds of new stimulation around here.
Midday update (Thursday 1/22)
Great news today: the preliminary report from Max's MRI came back this morning. The early report is that the brain tissue around Max's ventricles was not damaged by the swelling of the ventricles or the small leak one of his ventricles developed. More technically, Max does not have PVL (warning: scary link). Carolyn asked Dr. B.--who gave her the news--whether this meant we could relax. (By the way, has President Obama appointed a Surgeon General yet? If not, I nominate Dr. B.) The answer is that there's a small chance (10 percent) that Max could develop PVL in the future as his ventricles change shape. If they shrink rapidly, for example, the surrounding brain tissue could tear. In addition, we don't have the formal report from the radiologists. But Dr. B. isn't one to sit on good news.
Although Max did eventually tolerate his feeds when they were compressed to 90 minutes, the NICU team have decided to give him a break and slow the feeds down so they go in over 105 minutes instead. Max did vomit and desat when they first moved him to a 90 minute feed. Although he shows no signs of lung damage as a result, they are taking a less aggressive course in response. Carolyn asked why and was told "because we want him to succeed". The NICU team also discussed whether we'd be comfortable taking Max home with a feeding tube in case he couldn't get all of his nutrition orally. However, it looks like Max has at least another couple of weeks in the hospital to look forward to.
In sadder news, tomorrow is Dr. B.'s last day on rotation as the NICU attending. She has become our favorite physician of all time. We know the incoming attendings and they are formidable intellectuals covered in professional glory. I hope that they continue Dr. B.'s tradition of giving us excellent news.
Although Max did eventually tolerate his feeds when they were compressed to 90 minutes, the NICU team have decided to give him a break and slow the feeds down so they go in over 105 minutes instead. Max did vomit and desat when they first moved him to a 90 minute feed. Although he shows no signs of lung damage as a result, they are taking a less aggressive course in response. Carolyn asked why and was told "because we want him to succeed". The NICU team also discussed whether we'd be comfortable taking Max home with a feeding tube in case he couldn't get all of his nutrition orally. However, it looks like Max has at least another couple of weeks in the hospital to look forward to.
In sadder news, tomorrow is Dr. B.'s last day on rotation as the NICU attending. She has become our favorite physician of all time. We know the incoming attendings and they are formidable intellectuals covered in professional glory. I hope that they continue Dr. B.'s tradition of giving us excellent news.
Wednesday, January 21, 2009
Evening update (Wednesday 1/21)
The NICU team are slowly compressing Max's feeds over a shorter and shorter period of time. If his reflux causes him to vomit too much of his food back up when it's given over a 30 minute period, he's a candidate for a type of surgery. In addition, Max used to have a habit of inhaling his refluxed milk and damaging his lungs. Reflux itself can be painful for babies and parents alike of course, and maybe six months from now we'll be wishing he'd had the surgery. But right now, if he doesn't gain enough control over his esophagus, trachea and epiglottis, he'll need a semi-permanent feeding tube installed in his stomach, something we consider worse than reflux-induced crying (right now.)
The early results of Max's compressed feedings are mixed but, on balance, positive so far. He was in distress for the first few feedings after they moved from a continuous drip to 120 minutes. And after they moved to 90 minutes this morning Max vomited up 20 ccs of milk. However, after a late night phone call to the NICU, we learnt that Max has tolerated his most recent feeds well, with, at most, a "wet burp." Who doesn't have at least one wet burp per day? (Men only, please.)
No results yet from Max's 4:00 AM MRI. We did learn that they like to give MRIs in the dead of night because they're less likely to have to sedate the baby (Carolyn adds, "only if the baby knows night from day.")
PS All the links in the first paragraph came from Googling "my crying infant is driving me crazy." Some day, Max may very well drive us crazy with his incessant crying. We'd like to give him that chance, though.
The early results of Max's compressed feedings are mixed but, on balance, positive so far. He was in distress for the first few feedings after they moved from a continuous drip to 120 minutes. And after they moved to 90 minutes this morning Max vomited up 20 ccs of milk. However, after a late night phone call to the NICU, we learnt that Max has tolerated his most recent feeds well, with, at most, a "wet burp." Who doesn't have at least one wet burp per day? (Men only, please.)
No results yet from Max's 4:00 AM MRI. We did learn that they like to give MRIs in the dead of night because they're less likely to have to sedate the baby (Carolyn adds, "only if the baby knows night from day.")
PS All the links in the first paragraph came from Googling "my crying infant is driving me crazy." Some day, Max may very well drive us crazy with his incessant crying. We'd like to give him that chance, though.
Tuesday, January 20, 2009
Evening Update (Tuesday 1/20)
I think this might be the longest Carolyn and I have spent away from the hospital. We called a few times over the course of the day and heard quite a din in the background. It seems that the NICU is full of babies right now. (The nurses report that Max wasn't one of the crying infants in the background). Max continues to have pretty severe reflux, but his breathing remains pretty easy. In addition, after last night's eight hour marathon session of being awake and uncomfortable, Max had a more balanced day today, with typical infant waking and sleeping. One of the residents phoned in the middle of President Obama's inaugural address to request consent for an MRI. Max had been scheduled to have one this week. I heard the new president in one early and the resident in the other talking about how the MRI lab was strangely empty and this was our golden opportunity to get Max in. This is just a routine evaluation that the NICU team does on all babies at this point in their stay, but my guess is that scheduling a routine MRI is hard because it's always getting bumped in favor of the emergency cases. The resident knew a good bet when she saw one, although I wonder if she quite knew why the demand for elective medcial procedures was so low. No word on whether Max actually got his MRI today. And from what I could tell, I'm better off waiting for this president's second inaugural anyway.
Monday, January 19, 2009
Evening update (Monday 1/19)
Carolyn spent the day with Max and we just phoned the NICU to get the late night update. In sum, it seems that Max is in some discomfort, probably because of his reflux, but his breathing continues to be relatively easy with no desats. Nurse C. reports that Max has been continuously awake for the past eight hours--a very long stretch for a baby (indeed, for his parents).
We will check in by phone tomorrow but, because the bridges are closed, the hotels booked solid and the hospital full of grumpy nurses and doctors forced to overnight during the inaguration, we're probably not going to make it in tomorrow.
We will check in by phone tomorrow but, because the bridges are closed, the hotels booked solid and the hospital full of grumpy nurses and doctors forced to overnight during the inaguration, we're probably not going to make it in tomorrow.
Sunday, January 18, 2009
Evening update (Sunday 1/18)
I told Carolyn that she would have to begin her description of the day this way: "As I drove to Georgetown under leaden skies with the constant drone of unseen helicopters..." but she said that was no way to describe Washington this weekend. True, the weather isn't great, and the security precautions have to be seen to be believed, but the city is full of happy people. Carolyn got caught in a mysterious traffic jam this morning; the Post website carried the pictures of the big party on the Mall.
Today was Max's first day back on a compressed feeding schedule; the NICU team are starting him off slowly with his feeds compressed to two hours every three hours--just barely faster than the continuous drip he'd been getting before. Carolyn reports that he had a few very brief desats but was otherwise breathing easily. We've gotten used to seeing Max go hours and hours without a desat, so this was a little disheartening. Nonetheless, Max's breathing is much easier than it was a week ago. We're hoping he gets the hang of keeping his food out of his lungs.
In other news, Carolyn concedes that Max's eyes aren't blue anymore, but she thinks they haven't settled down yet. They'll either be grey or, possibly, hazel.
At the late night phone call we learnt from nurse C. that he is breathing easily with no desats. She gave him a bath ("he was mad at me!") and then fell asleep.
Today was Max's first day back on a compressed feeding schedule; the NICU team are starting him off slowly with his feeds compressed to two hours every three hours--just barely faster than the continuous drip he'd been getting before. Carolyn reports that he had a few very brief desats but was otherwise breathing easily. We've gotten used to seeing Max go hours and hours without a desat, so this was a little disheartening. Nonetheless, Max's breathing is much easier than it was a week ago. We're hoping he gets the hang of keeping his food out of his lungs.
In other news, Carolyn concedes that Max's eyes aren't blue anymore, but she thinks they haven't settled down yet. They'll either be grey or, possibly, hazel.
At the late night phone call we learnt from nurse C. that he is breathing easily with no desats. She gave him a bath ("he was mad at me!") and then fell asleep.
Saturday, January 17, 2009
Evening update (Saturday 01/17)
Max had another good day today. He and nurse R. made me a heart-shaped card for my birthday; it also had a little bottle of nail polish in gift bag. (Max and nurse R. chose "I'm Not Really A Waitress", one of mommy's favorite colors now that she's safely out of graduate school and unlikely to be waitress.)
We spent the afternoon together, playing/exercising with a little nap worked in. His sats continue to be very high 90s or even 100 with few or no desats, and his respiratory rate is good. When he's awake he is getting better state control, that is, not freaking out at every movement. As you can see from the recent posts, we now even have video evidence of this.
Max's head circumference has now been stable at 39 cm for a few days. His weight tonight is 3700 grams, or a little over 8 lbs.
Tomorrow is a big day for Max. His feedings will start being compressed so that he is fed through the NG tube for 2 hours, then gets an hour break, then the 2-1 cycle repeats. We'll start to see whether his respiratory system can handle whatever reflux his body throws at it. We're all pulling for you, Max. Good luck.
We spent the afternoon together, playing/exercising with a little nap worked in. His sats continue to be very high 90s or even 100 with few or no desats, and his respiratory rate is good. When he's awake he is getting better state control, that is, not freaking out at every movement. As you can see from the recent posts, we now even have video evidence of this.
Max's head circumference has now been stable at 39 cm for a few days. His weight tonight is 3700 grams, or a little over 8 lbs.
Tomorrow is a big day for Max. His feedings will start being compressed so that he is fed through the NG tube for 2 hours, then gets an hour break, then the 2-1 cycle repeats. We'll start to see whether his respiratory system can handle whatever reflux his body throws at it. We're all pulling for you, Max. Good luck.
What color are those eyes?
Carolyn and I had a heated debate yesterday via text message about the color of Max's eyes. Carolyn thinks that they're still blue. I think that they were never the blue of an adult, that when Max was born 10 weeks early his eyes were passing through a phase not meant to be seen. To me, his eyes look dark violet, they were the unnerving eyes of a spaceman.
But now that Max has marked more then 12 weeks since he was born he's beginning to look like a real baby. In an attempt to bring some data to bear on the question, I offer two videos that Carolyn took at the NICU today. They both run about 90 seconds each, and feature close up and extreme close up shots of Max rolling his eyes. The videos also highlight the progress Max has made. He just looks like a normal baby. You can also hear the institutional din of a NICU in the background. None of the alarms going off pertain to Max.
But now that Max has marked more then 12 weeks since he was born he's beginning to look like a real baby. In an attempt to bring some data to bear on the question, I offer two videos that Carolyn took at the NICU today. They both run about 90 seconds each, and feature close up and extreme close up shots of Max rolling his eyes. The videos also highlight the progress Max has made. He just looks like a normal baby. You can also hear the institutional din of a NICU in the background. None of the alarms going off pertain to Max.
Sleeping Max
Sleeping Max
Originally uploaded by andreas.lehnert
Crib Tour
Crib Tour
Originally uploaded by andreas.lehnert
Friday, January 16, 2009
Evening Update (Friday 1/16)
Just like on airplanes, you're not allowed to use wireless devices in the NICU. As a matter of principle I'll follow any policy the NICU dictates. This evening, however, Carolyn and I conducted a serious debate via text message; to hold up my end I had to tap away surreptitiously, when the nurses weren't looking. We were discussing the color of Max's eyes while I was staring directly into them. I don't see how there could be serious debate when I was looking at them and Carolyn was four miles awa,y, feeding Felix dinner. My position is that Max's eyes are greenish-hazel; Carolyn thinks they're blue. We'll try to gather and present photographic evidence tomorrow.
Also, while I was with Max, he and the nurses showed me the present he's working on for Carolyn's birthday tomorrow. In case she doesn't like it, I got chocolates and flowers too.
Here in Washington we've got a four-day weekend coming up, and they're really serious about not letting anyone over the bridges on Monday, not even doctors and nurses. Thus, the whole NICU team that we've gotten used to are leaving tonight and not returning until Wednesday morning. Carolyn sat down with the sainted Dr. B. and talked over the plan for the next few days. Dr. B. assured Carolyn that she had written detailed instructions for Max's care and that she's sure that the attendings who make their way to the hospital in coming days will follow the plan. Max's digestive holiday is slated to end on Sunday, when he returns to "compressed feeds". At the moment he is being fed continuously at an ultra slow rate. Max gets the volume that babies are expected to eat in, at most, 30 minutes spread out over three hours. And because babies have to be fed every three hours this means that he is continuously being fed. Starting on Sunday his feedings will be compressed into...two hours. (Carolyn asked about started at 2.5 hours, but the NICU team thinks that would be just the same as his current schedule.) So Max's feeds won't be compressed by much, at least at first.
The NICU team put Max on the slow drip feeding schedule to give him time to get his nervous system a little more organized and to give his lungs a rest. Carolyn and I have both noticed that Max's breathing is quite easy and stable; far better than we've ever seen it. Indeed, when I was with him today I picked him up and, unthinkingly, put him up on my shoulder like I would a normal baby. Max was fine (he kind of enjoyed the view), but he's still trailing as many wires as an astronaut so I had to carefully untangle the lines I messed up. I think he's ready for the next challenge.
The doctors told Carolyn that Max's recent head growth is normal and that his head feels good. Max's skull is a little mis-shapen now, the result of spending too much time on the same side. Max prefers to look out at the NICU, so they've reversed the direction of the crib so he can look out at the world while lying on his other side.
Max had a session with physical therapist A. today. A. told Carolyn that a big part of physical therapy is helping a baby learn "state control". Some babies, when distressed, can freak themselves out and spiral into uncontrollable, self-perpetuating, crying. State control is the art of realizing that a small disturbance such as a loud noise, a dirty diaper or getting tangled up in monitor wires while your dad swears continuously does not mean the end of the world, that there's no need to panic because things will get better.
Also, while I was with Max, he and the nurses showed me the present he's working on for Carolyn's birthday tomorrow. In case she doesn't like it, I got chocolates and flowers too.
Here in Washington we've got a four-day weekend coming up, and they're really serious about not letting anyone over the bridges on Monday, not even doctors and nurses. Thus, the whole NICU team that we've gotten used to are leaving tonight and not returning until Wednesday morning. Carolyn sat down with the sainted Dr. B. and talked over the plan for the next few days. Dr. B. assured Carolyn that she had written detailed instructions for Max's care and that she's sure that the attendings who make their way to the hospital in coming days will follow the plan. Max's digestive holiday is slated to end on Sunday, when he returns to "compressed feeds". At the moment he is being fed continuously at an ultra slow rate. Max gets the volume that babies are expected to eat in, at most, 30 minutes spread out over three hours. And because babies have to be fed every three hours this means that he is continuously being fed. Starting on Sunday his feedings will be compressed into...two hours. (Carolyn asked about started at 2.5 hours, but the NICU team thinks that would be just the same as his current schedule.) So Max's feeds won't be compressed by much, at least at first.
The NICU team put Max on the slow drip feeding schedule to give him time to get his nervous system a little more organized and to give his lungs a rest. Carolyn and I have both noticed that Max's breathing is quite easy and stable; far better than we've ever seen it. Indeed, when I was with him today I picked him up and, unthinkingly, put him up on my shoulder like I would a normal baby. Max was fine (he kind of enjoyed the view), but he's still trailing as many wires as an astronaut so I had to carefully untangle the lines I messed up. I think he's ready for the next challenge.
The doctors told Carolyn that Max's recent head growth is normal and that his head feels good. Max's skull is a little mis-shapen now, the result of spending too much time on the same side. Max prefers to look out at the NICU, so they've reversed the direction of the crib so he can look out at the world while lying on his other side.
Max had a session with physical therapist A. today. A. told Carolyn that a big part of physical therapy is helping a baby learn "state control". Some babies, when distressed, can freak themselves out and spiral into uncontrollable, self-perpetuating, crying. State control is the art of realizing that a small disturbance such as a loud noise, a dirty diaper or getting tangled up in monitor wires while your dad swears continuously does not mean the end of the world, that there's no need to panic because things will get better.
Thursday, January 15, 2009
Evening update (Thursday 1/15)
A busy day for Max. He had speech therapy, physical therapy and of course the standard workout with his mother. Carolyn reports that his breathing seemed relatively easy today, with a respiratory rate well below the tachypnic levels from earlier this week. Max is going for longer and longer periods without setting off his oxygen saturation alarm. His monitor displays the time and severity of the four most recent such episodes. In the past few days we've noticed that the gap between the earliest and latest alarms shown has been growing. When Carolyn got to the NICU this morning, the oldest alarm was actually from the previous day.
Speech therapist S. arrived in the afternoon when Max was a little cranky. By that time, Max had had his vitamins and was fairly gassy. She spent a lot of time trying to calm Max down. Nonetheless, Max got some work done on his pacifier, and otherwise showed signs of oral competence.
Physical therapist J. arrived after Carolyn had been working with Max for half an hour. Max did well moving his head, cycling his legs and centering himself. Max had his monthly assessment, so J. checked the four reflexes of infancy and conducted other tests. The bottom line is that he's made a lot of progress. J. would like to see him move his head more but of course he has a very big head. His state control is better than before. They seem quite happy with his progress.
Speech therapist S. arrived in the afternoon when Max was a little cranky. By that time, Max had had his vitamins and was fairly gassy. She spent a lot of time trying to calm Max down. Nonetheless, Max got some work done on his pacifier, and otherwise showed signs of oral competence.
Physical therapist J. arrived after Carolyn had been working with Max for half an hour. Max did well moving his head, cycling his legs and centering himself. Max had his monthly assessment, so J. checked the four reflexes of infancy and conducted other tests. The bottom line is that he's made a lot of progress. J. would like to see him move his head more but of course he has a very big head. His state control is better than before. They seem quite happy with his progress.
Wednesday, January 14, 2009
Evening Update (Wednesday 1/14)
Another good day for Max overall. Carolyn reports that he was breathing a little fast, particularly towards the end of the day. In the past, this has been an early sign of respiratory distress. Oh, and one of the nurses measured Max's head today and found that it had grown + 1.0 cm in less than a day. Carolyn and I are completely inured to these kinds of head circumference measurement panics. We'll wait for the official estimate tonight before we leak a little adrenaline into our bloodstreams.
But aside from that, Max and Carolyn had a great day together. Carolyn only put Max through a partial workout in case one of the physical therapists wanted to work with him. However, she devised a modified tummy time exercise in which Carolyn reclines as much as the hospital rockers permit, puts Max face-down on her stomach and encourages him to move his head side to side, lift his head etc. It went quite well, Speech therapist S. dropped by and worked with Max. She report that Max did well with his pacifier.
The plan is to try Max with oral feeds late this week or early next. Carolyn got the impression that the NICU team think that Max's reflux will really flare up and that they will have to pursue "alternatives" (read: surgery on the pyloric valve). But at this point I've got my money on Max figuring it all out. He is, like his father and many other famous people, a slow learner.
It may be a sign of NICU fatigue, but Carolyn now thinks that the NICU team thinks she is spoiling Max by picking him up every time he starts to cry. (Earlier this week, Carolyn thought she had been marked out as a crazy NICU mom for insisting that the weekend NICU team feel Max's fontanels with the outgoing residents so they could compare notes and properly detect any changes.) My own view is that the NICU team have seen the entire spectrum of parental pathologies and that our behavior doesn't rate even a raised eyebrow. But back to the subject of "spoiling" babies: this was a debate that Carolyn and I read up on before Felix was born. It just seems so refreshingly normal to hear people argue attachment parenting vs. Ferberization. The last time we talked about this, we couldn't have told you where the pyloric valve was, or how to detect hydrocephalus, or even what chronic lung disease was. Battle of wills with the infant? Bring it on! (For the record, Carolyn and I are practicing orthodox Ferberarians, but we're ecumenical enough to allow attachment parenters into our house. When their coddled little darling throws a tantrum, however, out they go.)
But this brings me to another one of my crackpot parenting theories: in the same way that babies are hardwired to follow faces, I think that they are instinctive manipulators of adults. After all, the ability to get grown-ups to do what they wanted probably was a big help to babies back in the cave man days. So Max likely is trying to manipulate us, not to mention the whole NICU team. And that's great news! It means that part of that very big brain of his is starting to light up. As I reminded Carolyn, chances are we'll be able to outfox Max for a few years yet.
But aside from that, Max and Carolyn had a great day together. Carolyn only put Max through a partial workout in case one of the physical therapists wanted to work with him. However, she devised a modified tummy time exercise in which Carolyn reclines as much as the hospital rockers permit, puts Max face-down on her stomach and encourages him to move his head side to side, lift his head etc. It went quite well, Speech therapist S. dropped by and worked with Max. She report that Max did well with his pacifier.
The plan is to try Max with oral feeds late this week or early next. Carolyn got the impression that the NICU team think that Max's reflux will really flare up and that they will have to pursue "alternatives" (read: surgery on the pyloric valve). But at this point I've got my money on Max figuring it all out. He is, like his father and many other famous people, a slow learner.
It may be a sign of NICU fatigue, but Carolyn now thinks that the NICU team thinks she is spoiling Max by picking him up every time he starts to cry. (Earlier this week, Carolyn thought she had been marked out as a crazy NICU mom for insisting that the weekend NICU team feel Max's fontanels with the outgoing residents so they could compare notes and properly detect any changes.) My own view is that the NICU team have seen the entire spectrum of parental pathologies and that our behavior doesn't rate even a raised eyebrow. But back to the subject of "spoiling" babies: this was a debate that Carolyn and I read up on before Felix was born. It just seems so refreshingly normal to hear people argue attachment parenting vs. Ferberization. The last time we talked about this, we couldn't have told you where the pyloric valve was, or how to detect hydrocephalus, or even what chronic lung disease was. Battle of wills with the infant? Bring it on! (For the record, Carolyn and I are practicing orthodox Ferberarians, but we're ecumenical enough to allow attachment parenters into our house. When their coddled little darling throws a tantrum, however, out they go.)
But this brings me to another one of my crackpot parenting theories: in the same way that babies are hardwired to follow faces, I think that they are instinctive manipulators of adults. After all, the ability to get grown-ups to do what they wanted probably was a big help to babies back in the cave man days. So Max likely is trying to manipulate us, not to mention the whole NICU team. And that's great news! It means that part of that very big brain of his is starting to light up. As I reminded Carolyn, chances are we'll be able to outfox Max for a few years yet.
Tuesday, January 13, 2009
Evening Update (Tuesday 1/13)
More than 10 years ago, back when we were living in Chicago, a friend of ours had a kid who had to spend a couple of nights in the NICU. He described how many of the other babies in the NICU had parents who didn't seem to be around very much. These babies were not starved for human company however; the hospital had organized a team of volunteers to hold them, sing to them, and so on. So it was inevitable that, when Carolyn walked into the NICU this morning, Max was being held by a kindly volunteer. That wasn't the worst of it: Carolyn and I also had to hear all day long about what a great singer the volunteer was. It's possible that the NICU team were hinting to me that they could do without another rendition of "Snake Baked a Hoecake". They haven't heard me sing "This Ain't No Picnic".
Dr. B. cemented her position as our favorite NICU attending by saying that Max had had a great day. True, he did pull his NG tube out twice during the day, but he tolerated the tubes' reinsertion without complaint. (A few weeks ago, Max reacted to having a feeding tube inserted with a severe desat and associated brady; today he didn't bat an eye as far as we could tell.) Indeed, Max had the fewest desats in any 12 hour period that we can recall. He did gain 180 grams overnight, which is an unusual amount and might signal some fluid retention. However, he didn't look puffy and his lungs certainly weren't in distress. Dr. B. suggested that it was just normal growth, putting her in the running for our award for favorite doctor of all time.
Max didn't have a scheduled physical therapy session, but Carolyn worked out with him (something I didn't see any of the volunteers doing, no matter how great their singing voices). Carolyn reports that Max wants to do head lifts even when they've moved on a different exercise. Max bicycled his own legs, and otherwise did extremely well. Indeed, at one point Max was crying lustily enough to attract the attention of physical therapist A., who was there working with another baby. A. rushed over and exclaimed on how much healthier Max looked to her.
At one point, Max was crying for a few minutes while Carolyn tried to console him. She noticed something strange in his eyes. She called over nurse R., who diagnosed the leakage as tears. Babies, of course, don't cry real tears until a few weeks after birth.
Dr. B. cemented her position as our favorite NICU attending by saying that Max had had a great day. True, he did pull his NG tube out twice during the day, but he tolerated the tubes' reinsertion without complaint. (A few weeks ago, Max reacted to having a feeding tube inserted with a severe desat and associated brady; today he didn't bat an eye as far as we could tell.) Indeed, Max had the fewest desats in any 12 hour period that we can recall. He did gain 180 grams overnight, which is an unusual amount and might signal some fluid retention. However, he didn't look puffy and his lungs certainly weren't in distress. Dr. B. suggested that it was just normal growth, putting her in the running for our award for favorite doctor of all time.
Max didn't have a scheduled physical therapy session, but Carolyn worked out with him (something I didn't see any of the volunteers doing, no matter how great their singing voices). Carolyn reports that Max wants to do head lifts even when they've moved on a different exercise. Max bicycled his own legs, and otherwise did extremely well. Indeed, at one point Max was crying lustily enough to attract the attention of physical therapist A., who was there working with another baby. A. rushed over and exclaimed on how much healthier Max looked to her.
At one point, Max was crying for a few minutes while Carolyn tried to console him. She noticed something strange in his eyes. She called over nurse R., who diagnosed the leakage as tears. Babies, of course, don't cry real tears until a few weeks after birth.
Monday, January 12, 2009
Evening Update (Monday 1/12)
Lots to report today. I'll start with a recap of Carolyn's very nice day at the NICU, and then discuss medical developments, the treatment plan, and some advice we got from Dr. B., who is fast becoming our favorite attending. Readers who make it all the way to the end will get to find our why we're such big fans of Dr. B. and get some other welcome news.
Carolyn arrived this morning to find Max awake and alert in his frog chair (a bouncy seat). This is his usual routine: wake up quite early -- before the 7:00 AM shift change -- and spend the morning taking in the NICU from his chair. Carolyn spent some time playing with Max before he became drowsy and fell asleep again. Around 1:30 PM the NICU team pulled Max's ND tube back slightly so that it no longer terminates in the duodenum (the "D" in "ND"). Instead, it terminates in the stomach, making it a more normal NG tube ("G" for "gastric", I believe).
Physical therapist J. arrived a little later, and Max enjoyed another successful physical therapy session. He tolerated it well, tracked motion with his eyes and completed the usual routine of PT exercises. In the past, we've had trouble convincing Max to follow objects with his eyes. Physical therapist J. said that babies are much more likely to follow a face than anything else. I believe this is why infant toys often have stylized faces on them. She encouraged us to spend time playing, singing and otherwise interacting with Max when he is awake and alert. She emphasized that it's especially important to make eye contact with Max while we're playing with him.
After his workout, Max was quite alert. Carolyn followed J.'s advice and interacted with him. In addition, Max received a steady stream of visitors who dropped by to say hello. Max was very alert and focused for a couple of hours. The nurses tell us--and we've tried to resist facing up to this for as long as possible--that Max is uncomfortable when he has a load of stool in his diaper. This marks him as different from his brother and, indeed, his father and uncle. As the afternoon ended, Max was clearly bothered by something. It turned out to be a diaper full of stool.
One of Max's visitors this afternoon was Dr. Sh., one of the NICU fellows. We first met Dr. Sh. when the NICU team sent her over to see us while Carolyn was still pregnant, but in pre-term labor. She gave us what we recognized at the time as a standard what-to-expect-when-you're-expecting-way-too-early speech, a kind of harsh introduction to the NICU that emphasized everything that could go wrong in premature babies. Dr. Sh. told us then that preemies had trouble with their lungs, that they were prone to head bleeds and that they could have gastric problems. She also told us that we could expect the NICU to hold the twins for seven weeks before sending them home with us. The speech left Carolyn and me suitably terrified. Since then, we've come to know Dr. Sh. as a caring and humane doctor, and someone we can work with quite well.
Because the NICU team rotates their schedules over weekends, Carolyn makes sure to find someone on Friday who will at least overlap wth the weekend team to feel Max's fontanels so they can gauge whether Max's head changes over the weekend. (Carolyn told me that she feels that the NICU team thinks has become a crazy NICU mom.) Dr. Sh. was one of the group Carolyn drafted to keep continuity of care for Max's head over the weekend.
But I actually think Dr. Sh. dropped by because Max is one of the most popular babies in the NICU. Of course, we think Max is incredibly cute (pictures don't do him justice) and has a winning personality. But even beyond these elements of charisma, I think that the NICU team love to see what they consider a true NICU success story; they can look at Max and feel good about all of the work they've done over the past few months. I continue to believe that, although the NICU team are marvellous, the babies do all the actual work.
With the ND tube now replaced by a NG tube, Max faces another test of his abilities. Will he be able to control his esophagus and associated muscles properly so that he doesn't breathe in the milk he refluxes back up? The NICU team believe that this kind of aspiration caused his earlier breathing difficulties, and indeed since they moved to an ND tube (from which milk cannot, in principle, escape) his breathing has become a lot stronger. If Max can keep from stressing out his lungs too much, the NICU team will gradually reintroduce a standard feeding schedule. (He's currently on a continuous slow drip.) If Max can't control his eating, the NICU team will consider other alternatives, some of which involve fairly drastic surgery.
Carolyn spoke with the attending, Dr. B., again today. Dr. B. is fast becoming our favorite NICU doc. She apparently does not subscribe to the quasi-religious attitude of extreme pessimism favored by the other NICU attendings. She told Carolyn that, over the week she has treated him, Max has become a "different baby"--he is stronger, has better color, and is more stable. She also told Carolyn that it is time "to quit waiting for the other shoe to drop."
Along those lines, Carolyn spoke to the NICU tonight. Max has handled his first 10 hours back on an NG tube quite well, with no desats, not to mention episodes of apneas or bradycardia. In addition, nurse K. measured his head circumference and found that it had dropped -0.5 cm from last night, leaving it at 37.5 cm.
Carolyn arrived this morning to find Max awake and alert in his frog chair (a bouncy seat). This is his usual routine: wake up quite early -- before the 7:00 AM shift change -- and spend the morning taking in the NICU from his chair. Carolyn spent some time playing with Max before he became drowsy and fell asleep again. Around 1:30 PM the NICU team pulled Max's ND tube back slightly so that it no longer terminates in the duodenum (the "D" in "ND"). Instead, it terminates in the stomach, making it a more normal NG tube ("G" for "gastric", I believe).
Physical therapist J. arrived a little later, and Max enjoyed another successful physical therapy session. He tolerated it well, tracked motion with his eyes and completed the usual routine of PT exercises. In the past, we've had trouble convincing Max to follow objects with his eyes. Physical therapist J. said that babies are much more likely to follow a face than anything else. I believe this is why infant toys often have stylized faces on them. She encouraged us to spend time playing, singing and otherwise interacting with Max when he is awake and alert. She emphasized that it's especially important to make eye contact with Max while we're playing with him.
After his workout, Max was quite alert. Carolyn followed J.'s advice and interacted with him. In addition, Max received a steady stream of visitors who dropped by to say hello. Max was very alert and focused for a couple of hours. The nurses tell us--and we've tried to resist facing up to this for as long as possible--that Max is uncomfortable when he has a load of stool in his diaper. This marks him as different from his brother and, indeed, his father and uncle. As the afternoon ended, Max was clearly bothered by something. It turned out to be a diaper full of stool.
One of Max's visitors this afternoon was Dr. Sh., one of the NICU fellows. We first met Dr. Sh. when the NICU team sent her over to see us while Carolyn was still pregnant, but in pre-term labor. She gave us what we recognized at the time as a standard what-to-expect-when-you're-expecting-way-too-early speech, a kind of harsh introduction to the NICU that emphasized everything that could go wrong in premature babies. Dr. Sh. told us then that preemies had trouble with their lungs, that they were prone to head bleeds and that they could have gastric problems. She also told us that we could expect the NICU to hold the twins for seven weeks before sending them home with us. The speech left Carolyn and me suitably terrified. Since then, we've come to know Dr. Sh. as a caring and humane doctor, and someone we can work with quite well.
Because the NICU team rotates their schedules over weekends, Carolyn makes sure to find someone on Friday who will at least overlap wth the weekend team to feel Max's fontanels so they can gauge whether Max's head changes over the weekend. (Carolyn told me that she feels that the NICU team thinks has become a crazy NICU mom.) Dr. Sh. was one of the group Carolyn drafted to keep continuity of care for Max's head over the weekend.
But I actually think Dr. Sh. dropped by because Max is one of the most popular babies in the NICU. Of course, we think Max is incredibly cute (pictures don't do him justice) and has a winning personality. But even beyond these elements of charisma, I think that the NICU team love to see what they consider a true NICU success story; they can look at Max and feel good about all of the work they've done over the past few months. I continue to believe that, although the NICU team are marvellous, the babies do all the actual work.
With the ND tube now replaced by a NG tube, Max faces another test of his abilities. Will he be able to control his esophagus and associated muscles properly so that he doesn't breathe in the milk he refluxes back up? The NICU team believe that this kind of aspiration caused his earlier breathing difficulties, and indeed since they moved to an ND tube (from which milk cannot, in principle, escape) his breathing has become a lot stronger. If Max can keep from stressing out his lungs too much, the NICU team will gradually reintroduce a standard feeding schedule. (He's currently on a continuous slow drip.) If Max can't control his eating, the NICU team will consider other alternatives, some of which involve fairly drastic surgery.
Carolyn spoke with the attending, Dr. B., again today. Dr. B. is fast becoming our favorite NICU doc. She apparently does not subscribe to the quasi-religious attitude of extreme pessimism favored by the other NICU attendings. She told Carolyn that, over the week she has treated him, Max has become a "different baby"--he is stronger, has better color, and is more stable. She also told Carolyn that it is time "to quit waiting for the other shoe to drop."
Along those lines, Carolyn spoke to the NICU tonight. Max has handled his first 10 hours back on an NG tube quite well, with no desats, not to mention episodes of apneas or bradycardia. In addition, nurse K. measured his head circumference and found that it had dropped -0.5 cm from last night, leaving it at 37.5 cm.
Sunday, January 11, 2009
Max pulls on his ND tube
Max pulls on his ND tube
Originally uploaded by andreas.lehnert
Head lifts
Head lifts
Originally uploaded by andreas.lehnert
Friday, January 9, 2009
Evening Update (Friday 1/9)
(Late night update: Nurse N. reports Max's sats are holding up and she measured his head circumference at 38.0 cm, down -0.5 cm from yesterday.)
Today Max marked his 11th week in the NICU, or the first week since his original due date. Carolyn arrived at the NICU this morning to find Max wide awake and alert in his bouncy seat, sucking on his pacifier. Nurse J. reported that Max had been awake since before the start of her 7:00 AM shift. Carolyn did a full set of physical therapy exercises with Max, including head lifts, bicycles and a new arm exercise Carolyn has developed that she refers to as the "stretch--and then center". Carolyn saved for last the exercises that require Max to be fully cuddled (the others take place with Max on Carolyn's lap). In the middle of second rep, Max conked out completely and fell deeply asleep. For the rest of the day he was quite sleepy.
Carolyn and I both noticed that Max's breathing seemed much easier today. His oxygen saturation measurements were in the high 90s continuously while I was there (and I normally cause him to have at least one desat). The alarm record on his monitor showed that he's going up to two or three hours between desats, and even those are relatively mild. The docs are pleased with Max's respiratory performance off the cannula, and attribute its success to his steady dose of a diuretic (aldactazide).
In other news, our friend D. visited Max today and the two of them hit it off immediately. D. has skills as a baby whisperer that are eerie to behold. She clucked at a sleeping Max and his eyes popped wide open and he stared at her in total fascination.
The main medical issue we've been worrying about over the past few days is the acceleration in the growth of Max's head. In addition, Max's fontanels "feel full". Personally, I'm too scared to palpitate Max's head, but Carolyn, the docs and the nurses agree that they can feel more fluid through Max's fontanels. All of this suggests that we might be seeing a return of Max's hydrocephalus, something we were starting to think he'd managed to shake off. As a precaution, the NICU team ordered a head ultrasound, or HUS. The results of the HUS showed that Max's ventricles were stable; that is, that they hadn't swollen further. Max's ventricles stopped growing at about the same time that his head circumference settled down. This is evidence (we think) that whatever is going on, it isn't a dramatic resurgence of Max's hydrocephalus.
Dr. B., the attending, thinks that Max's head growth is perfectly normal. She told Carolyn today that babies' heads typically experience a growth spurt between one and three weeks after birth (one presumes that this is different from the rebound in a baby's skull following its compression during labor itself). Further, the timing of this growth spurt is, Dr. B. said, associated with gestational age as opposed to calendar age. Thus, although Max is 11 weeks old, he's only one week past his due date, putting him in the prime age bracket for a head growth spurt.
Carolyn asked why babies' heads grow so quickly at that stage. My theory--which Carolyn advanced to Dr. B.--was that it had something to do with bone growth as the fontanels closed. Dr. B. said it wasn't bone that was growing; she said that it was babies' brains that were growing.
Today Max marked his 11th week in the NICU, or the first week since his original due date. Carolyn arrived at the NICU this morning to find Max wide awake and alert in his bouncy seat, sucking on his pacifier. Nurse J. reported that Max had been awake since before the start of her 7:00 AM shift. Carolyn did a full set of physical therapy exercises with Max, including head lifts, bicycles and a new arm exercise Carolyn has developed that she refers to as the "stretch--and then center". Carolyn saved for last the exercises that require Max to be fully cuddled (the others take place with Max on Carolyn's lap). In the middle of second rep, Max conked out completely and fell deeply asleep. For the rest of the day he was quite sleepy.
Carolyn and I both noticed that Max's breathing seemed much easier today. His oxygen saturation measurements were in the high 90s continuously while I was there (and I normally cause him to have at least one desat). The alarm record on his monitor showed that he's going up to two or three hours between desats, and even those are relatively mild. The docs are pleased with Max's respiratory performance off the cannula, and attribute its success to his steady dose of a diuretic (aldactazide).
In other news, our friend D. visited Max today and the two of them hit it off immediately. D. has skills as a baby whisperer that are eerie to behold. She clucked at a sleeping Max and his eyes popped wide open and he stared at her in total fascination.
The main medical issue we've been worrying about over the past few days is the acceleration in the growth of Max's head. In addition, Max's fontanels "feel full". Personally, I'm too scared to palpitate Max's head, but Carolyn, the docs and the nurses agree that they can feel more fluid through Max's fontanels. All of this suggests that we might be seeing a return of Max's hydrocephalus, something we were starting to think he'd managed to shake off. As a precaution, the NICU team ordered a head ultrasound, or HUS. The results of the HUS showed that Max's ventricles were stable; that is, that they hadn't swollen further. Max's ventricles stopped growing at about the same time that his head circumference settled down. This is evidence (we think) that whatever is going on, it isn't a dramatic resurgence of Max's hydrocephalus.
Dr. B., the attending, thinks that Max's head growth is perfectly normal. She told Carolyn today that babies' heads typically experience a growth spurt between one and three weeks after birth (one presumes that this is different from the rebound in a baby's skull following its compression during labor itself). Further, the timing of this growth spurt is, Dr. B. said, associated with gestational age as opposed to calendar age. Thus, although Max is 11 weeks old, he's only one week past his due date, putting him in the prime age bracket for a head growth spurt.
Carolyn asked why babies' heads grow so quickly at that stage. My theory--which Carolyn advanced to Dr. B.--was that it had something to do with bone growth as the fontanels closed. Dr. B. said it wasn't bone that was growing; she said that it was babies' brains that were growing.
Thursday, January 8, 2009
Afternoon update (Thursday 1/8)
(Late night update: Head circumference now up to 38.5 cm, but nurse H. reports that otherwise Max is doing okay tonight.)
Carolyn called with an update from the NICU. She said that his head still felt full, i.e. she could feel more fluid under his fontanel than we've seen in the past. The nurses remeasured his head circumference a couple of times last night to see if perhaps it would fall, or they had mismeasured it, but to no avail. He's 38 cm around and that's solid. So there's something going on in there. Carolyn wondered if he might be starting to get interested and curious about the world around him, and his brain was expanding to accommodate all the extra thinking he was doing.
Indeed, Max seemed very engaged in the world around him today. Reports are that he spent the morning outside of his crib, in his bouncy seat, and was awake the whole time. He had a great physical therapy session this afternoon: he lifted his head, he followed sounds and motion, he brought his arms up to his chest--all the things that babies are supposed to do. Physical therapist J. also told Carolyn that it was perfectly normal, and indeed a good sign, for Max's arms and legs to sometimes be tense and other times to be relaxed. Problem babies sometimes are always tense or always floppy. Although I don't think Max had a speech therapy session, he sucked enthusiastically on his pacifier.
Max's breathing continued to seem easier, despite the greater demands on his system today. (The bouncy seat and physical therapy are hard work for babies.) Carolyn reports that his breathing rate was mostly moderate, and never escalated into the 100 breaths-per-minute range that we've sometimes seen. Although he sometimes "retracted" (i.e. visibly labored at breathing) it was never for long.
Nurse M. also administered his vitamins orally--a foul-smelling concoction. He spit the vitamins back up, along with some milk. (To be clear, I'm using "spit" in the way that parents, athletes and models do: to mean "vomit".) Of course, Max's stomach isn't supposed to have any milk in it because his feeding tube now goes past the stomach and terminates in the duodenum. How did milk make its way back up to the stomach? It's a mystery, and it elicited some truly odd theories from the NICU team, but it doesn't seem like a big deal.
So has Max's hydrocephalus come back? Somethings going on inside his skull. But he's not showing the classic signs of hydrocephalus, including "sunsetting"--having eyes chronically half-lidded. Indeed, he was bright eyed for much of the day. We'll just have to watch each night's head circumference reading closely. While we're waiting to see how this evolves, Max is becoming cuter and more engaged with the world every day.
Carolyn called with an update from the NICU. She said that his head still felt full, i.e. she could feel more fluid under his fontanel than we've seen in the past. The nurses remeasured his head circumference a couple of times last night to see if perhaps it would fall, or they had mismeasured it, but to no avail. He's 38 cm around and that's solid. So there's something going on in there. Carolyn wondered if he might be starting to get interested and curious about the world around him, and his brain was expanding to accommodate all the extra thinking he was doing.
Indeed, Max seemed very engaged in the world around him today. Reports are that he spent the morning outside of his crib, in his bouncy seat, and was awake the whole time. He had a great physical therapy session this afternoon: he lifted his head, he followed sounds and motion, he brought his arms up to his chest--all the things that babies are supposed to do. Physical therapist J. also told Carolyn that it was perfectly normal, and indeed a good sign, for Max's arms and legs to sometimes be tense and other times to be relaxed. Problem babies sometimes are always tense or always floppy. Although I don't think Max had a speech therapy session, he sucked enthusiastically on his pacifier.
Max's breathing continued to seem easier, despite the greater demands on his system today. (The bouncy seat and physical therapy are hard work for babies.) Carolyn reports that his breathing rate was mostly moderate, and never escalated into the 100 breaths-per-minute range that we've sometimes seen. Although he sometimes "retracted" (i.e. visibly labored at breathing) it was never for long.
Nurse M. also administered his vitamins orally--a foul-smelling concoction. He spit the vitamins back up, along with some milk. (To be clear, I'm using "spit" in the way that parents, athletes and models do: to mean "vomit".) Of course, Max's stomach isn't supposed to have any milk in it because his feeding tube now goes past the stomach and terminates in the duodenum. How did milk make its way back up to the stomach? It's a mystery, and it elicited some truly odd theories from the NICU team, but it doesn't seem like a big deal.
So has Max's hydrocephalus come back? Somethings going on inside his skull. But he's not showing the classic signs of hydrocephalus, including "sunsetting"--having eyes chronically half-lidded. Indeed, he was bright eyed for much of the day. We'll just have to watch each night's head circumference reading closely. While we're waiting to see how this evolves, Max is becoming cuter and more engaged with the world every day.
Wednesday, January 7, 2009
Evening update (Wednesday 1/7)
Tonight after we put Felix to bed, Carolyn opened the fridge and found a home-made shepherd's pie that had somehow wound up in our house. I know it was a shepherd's pie because it said so in a neatly hand-lettered label on a piece of masking tape on top of the container. We both had vague and conflicting memories of who made it and how (and when!) it came into our house, but we couldn't quite remember the exact details. Nonetheless, we heated it up for dinner. Mystery cook, your shepherd's pie was delicious, and saved us a great deal of trouble tonight. Many thanks, secret benefactor.
The NICU team--not a group of people given to false cheer--has assured us that Max's hydrocephalus appears to be resolving itself. However, the recent acceleration in his head growth has us naturally quite worried. It does no good for our habit of magical thinking to have Max's hydrocephalus resurge at precisely the same moment we had started to relax about it. I hope that Max is just having a growth spurt, a growth spurt that just happened to start with his head.
This morning I talked to Carolyn and she had only continued bad news to report about the evolution of Max's breathing problems. But when we spoke again in the afternoon, she was more upbeat. Dr. B. confirmed that Max has chronic lung disease, which appears to be more a label for the constellation of symptoms afflicting Max than a description of a specific underlying physical process. Dr. B. thinks that Max's lungs were damaged by the ventilator and oxygen support he got while very young. The good news is that, according to Dr. B., Max only has a mild case of it. Further, she expected that Max would not need to go back on the cannula, and she characterized the run of trouble Max has had this week just a "temporary setback".
Dr. B. also debunked my "buffer stock theory of breathing", where I thought that perhaps Max's lungs were only able to supply him with, say, 95% of his required oxygen. But, I thought, Max had built up a little extra buffer stock of oxygen while on the cannula. When the NICU team took the cannula away on Sunday, Max was able to draw on this buffer to augment his insufficient respiration for a couple of days. But by Tuesday, he had run down his buffer, and was struggling to get by on just his inadequate breathing, hence the tachypnia and retraction. Dr. B. assured Carolyn that Max has sufficient respiratory capacity for all the normal tasks a baby has to get done in a busy day: sleeping, eating, waving arms and legs around, pooping, being cute etc. Max, however, has a relatively small margin of extra capacity, so when stressed out, say by illness or fluid retention, it's more likely that he will experience respiratory distress.
As if to confirm Dr. B.'s diagnosis, Max perked up in the afternoon. In fact, Carolyn judged his respiratory situation to be good enough to get him out of his crib and play with him. Max was alert -- "bright eyed" -- and interested in the world around him. Carolyn got him to do three reps of our favorite new exercise: the head lift. Carolyn holds him sitting up, with his head flopped back. She then tickles his chest or back, and Max raises his head and brings his arms up. Given Max's enormous head, this is quite an effort. Dr Kz., the developmental specialist, gave Max a poor grade because his limbs were stronger than his trunk--these exercises strengthen his trunk. Max also sucked on his pacifier voluntarily. Speech therapist S. warned us not to force the pacifier on him, because it might make him pacifier-averse, so now give Max an infant Miranda warning when we try to interest him in a pacifier ("You do not have to suck on this pacifier...").
The NICU team--not a group of people given to false cheer--has assured us that Max's hydrocephalus appears to be resolving itself. However, the recent acceleration in his head growth has us naturally quite worried. It does no good for our habit of magical thinking to have Max's hydrocephalus resurge at precisely the same moment we had started to relax about it. I hope that Max is just having a growth spurt, a growth spurt that just happened to start with his head.
This morning I talked to Carolyn and she had only continued bad news to report about the evolution of Max's breathing problems. But when we spoke again in the afternoon, she was more upbeat. Dr. B. confirmed that Max has chronic lung disease, which appears to be more a label for the constellation of symptoms afflicting Max than a description of a specific underlying physical process. Dr. B. thinks that Max's lungs were damaged by the ventilator and oxygen support he got while very young. The good news is that, according to Dr. B., Max only has a mild case of it. Further, she expected that Max would not need to go back on the cannula, and she characterized the run of trouble Max has had this week just a "temporary setback".
Dr. B. also debunked my "buffer stock theory of breathing", where I thought that perhaps Max's lungs were only able to supply him with, say, 95% of his required oxygen. But, I thought, Max had built up a little extra buffer stock of oxygen while on the cannula. When the NICU team took the cannula away on Sunday, Max was able to draw on this buffer to augment his insufficient respiration for a couple of days. But by Tuesday, he had run down his buffer, and was struggling to get by on just his inadequate breathing, hence the tachypnia and retraction. Dr. B. assured Carolyn that Max has sufficient respiratory capacity for all the normal tasks a baby has to get done in a busy day: sleeping, eating, waving arms and legs around, pooping, being cute etc. Max, however, has a relatively small margin of extra capacity, so when stressed out, say by illness or fluid retention, it's more likely that he will experience respiratory distress.
As if to confirm Dr. B.'s diagnosis, Max perked up in the afternoon. In fact, Carolyn judged his respiratory situation to be good enough to get him out of his crib and play with him. Max was alert -- "bright eyed" -- and interested in the world around him. Carolyn got him to do three reps of our favorite new exercise: the head lift. Carolyn holds him sitting up, with his head flopped back. She then tickles his chest or back, and Max raises his head and brings his arms up. Given Max's enormous head, this is quite an effort. Dr Kz., the developmental specialist, gave Max a poor grade because his limbs were stronger than his trunk--these exercises strengthen his trunk. Max also sucked on his pacifier voluntarily. Speech therapist S. warned us not to force the pacifier on him, because it might make him pacifier-averse, so now give Max an infant Miranda warning when we try to interest him in a pacifier ("You do not have to suck on this pacifier...").
Tuesday, January 6, 2009
Evening update (Tuesday 1/6)
After a couple of days of breathing well on his own, Max started to run into trouble today. Carolyn spent the day with him, and noticed that he was breathing faster and "retracting"--i.e. breathing so hard that you can see his chest heaving. We spoke with Nurse B. who told us that Max's breathing problems persisted into the evening, with his breathing rate going over 100 breaths per minute. Although his oxygen saturation remained good, it was obvious that Max was working really hard to breathe. Nurse B. also thought Max looked a little puffier tonight than the last couple of nights.
In response, the NICU team hit Max with another dose of Lasix, and it seems to have given him some relief: his breathing rate is now down in the 40s, or even lower. We'll get a reading on whether Max is still retracting at the 3:30 AM check-in.
Max's head circumference increased another 0.5 cm, to 38 cm. The NICU attending examined his head and fontanels, and thought that they felt fine. She declared that "Max needs to grow."
In response, the NICU team hit Max with another dose of Lasix, and it seems to have given him some relief: his breathing rate is now down in the 40s, or even lower. We'll get a reading on whether Max is still retracting at the 3:30 AM check-in.
Max's head circumference increased another 0.5 cm, to 38 cm. The NICU attending examined his head and fontanels, and thought that they felt fine. She declared that "Max needs to grow."
Monday, January 5, 2009
Late night update (Monday 1/5)
Max had quite an adventure today: He took a bath in his spa, but, after his bath, while his head was still covered in shampoo, Nurse M. took him out of the step-down NICU to the staging area between the critical-care and step-down rooms where there's a deep sink with a warm-water tap. She rinsed off Max's head in this sink, where he attracted a lot of attention from his former neighbors in the critical-care room, who were able to see him through the glass walls.
Max also had an echocardiogram, which is a sonogram of his heart. It turns out that, several months ago, the NICU team had found a problem with Max's heart. We had forgotten all about it: there was a lot going on at the time and it was tough to keep track of all of Max's issues. Today's echo showed that Max's original problem has evolved into something less serious; the NICU team expect it resolve by itself. All of the technical terms flew past us, but this seems to be the upshot of today's test.
Max also had his regularly scheduled head ultrasound today; they were prepping him for it when I left at 7:00 PM. No word yet on the results.
Nurse B. was holding Max when Carolyn called a few minutes ago. While they were on the phone, Carolyn could hear Max cooing in the background. Nurse B. reports that Max was sucking heartily on his pacifier. This is something a lot of the night-time shift tell us, but that we don't get to see ourselves. Either they're better at getting Max to take a pacifier, or he's a nocturnal user. Carolyn did say that during the echocardiogram, Max was yelling and thrashing about until given a pacifier, which seemed to allow him to calm himself.
The NICU team took Max off of his cannula yesterday at noon, so he's been without respiratory support for almost a day and a half. He continues to keep his oxygen saturation levels steady in the mid-90s, with occasional but brief dips into the 80s or high 70s. The plan is to keep feeding him via a tube into his duodenum for a week to give his lungs a break from Max's habit of bringing up his stomach contents and breathing some of them back in. Next week they'll start working with Max to learn how to control his esophagus.
When I was at the NICU this evening I noticed that Carolyn had put another page from Where the Wild Things Are in Max's crib for him to look at. The first page Carolyn put up showed Max (the character) on a boat, travelling to the land of the wild things. You'll recall that Max lands on their shore:
Carolyn added the page where Max commands the wild things--despite their terrible roars, teeth and eyes--to be still.
Max also had an echocardiogram, which is a sonogram of his heart. It turns out that, several months ago, the NICU team had found a problem with Max's heart. We had forgotten all about it: there was a lot going on at the time and it was tough to keep track of all of Max's issues. Today's echo showed that Max's original problem has evolved into something less serious; the NICU team expect it resolve by itself. All of the technical terms flew past us, but this seems to be the upshot of today's test.
Max also had his regularly scheduled head ultrasound today; they were prepping him for it when I left at 7:00 PM. No word yet on the results.
Nurse B. was holding Max when Carolyn called a few minutes ago. While they were on the phone, Carolyn could hear Max cooing in the background. Nurse B. reports that Max was sucking heartily on his pacifier. This is something a lot of the night-time shift tell us, but that we don't get to see ourselves. Either they're better at getting Max to take a pacifier, or he's a nocturnal user. Carolyn did say that during the echocardiogram, Max was yelling and thrashing about until given a pacifier, which seemed to allow him to calm himself.
The NICU team took Max off of his cannula yesterday at noon, so he's been without respiratory support for almost a day and a half. He continues to keep his oxygen saturation levels steady in the mid-90s, with occasional but brief dips into the 80s or high 70s. The plan is to keep feeding him via a tube into his duodenum for a week to give his lungs a break from Max's habit of bringing up his stomach contents and breathing some of them back in. Next week they'll start working with Max to learn how to control his esophagus.
When I was at the NICU this evening I noticed that Carolyn had put another page from Where the Wild Things Are in Max's crib for him to look at. The first page Carolyn put up showed Max (the character) on a boat, travelling to the land of the wild things. You'll recall that Max lands on their shore:
And when he came to the place where the wild things are
they roared their terrible roars and gnashed their terrible teeth
and rolled their terrible eyes and showed their terrible claws
till Max said "BE STILL!"
and tamed them with the magic trick
Carolyn added the page where Max commands the wild things--despite their terrible roars, teeth and eyes--to be still.
Max's New Year's Resolutions
- To keep my head circumference growth stable and hydrocephalus in check
To breathe better and not scare my parents by turning blueAs of March 2009 this phase of Max's life appears to be behind him.- To learn to eat from a bottle and not need a tube into my duodenum
To be very, very cute(already done!)
Sunday, January 4, 2009
Going without a cannula (again)
Though bathtime is usually in the middle of the night, Max got a midday bath & shampoo today (for reasons that are still not clear to me) from Nurse M. This happened just before I arrived, and I was sorry to have missed it. We haven't seen Max get a bath since one time in early November. They took off Max's cannula today at noon to see how he would tolerate it. Max's nurse today seems to think that he has things too easy and that it is time for him to start experiencing new things ("peel my grapes" she said as she walked by him today). I suspect the cannula move was her idea. During my visit this afternoon from 1:30 - 5:30 p.m., he seemed to be doing well breathing on his own: no bradys, just one apnea (according to the monitor, but I was holding him and I could swear he was actually breathing), and his usual pattern of quick desats into the 80s and occasionally the high 70s. His typical sats were in the mid-90s, and his respiratory rate seemed pretty stable, with little retracting. Our phone call into the NICU tonight continues good news on the cannula-weaning front, as Max's breathing pattern continues to be pretty stable. This is the 4th effort they've made to take him off the cannula, so maybe the 4th time is the charm.
Max spent his time with me mostly sleeping, though he did wake up for some calisthenics and to receive his public (our friend Margaret stopped by for an afternoon visit). He seemed to tolerate the activity pretty well, only turning beet-red a few times. Tonight's head circumference measurement is the same as last night's (37.5 cm) and the nurse reports that his head feels good. I think a head ultrasound is scheduled for sometime this week (the last one was just before Christmas).
Max's new year's resolutions: (1) keep head circumference growth stable and hydrocephalus in check; (2) breathe better, and (3) get the ND tube out and learn to eat from a bottle.
Max spent his time with me mostly sleeping, though he did wake up for some calisthenics and to receive his public (our friend Margaret stopped by for an afternoon visit). He seemed to tolerate the activity pretty well, only turning beet-red a few times. Tonight's head circumference measurement is the same as last night's (37.5 cm) and the nurse reports that his head feels good. I think a head ultrasound is scheduled for sometime this week (the last one was just before Christmas).
Max's new year's resolutions: (1) keep head circumference growth stable and hydrocephalus in check; (2) breathe better, and (3) get the ND tube out and learn to eat from a bottle.
Saturday, January 3, 2009
On the tilted bed
Carolyn and I split the day at the NICU between us. I went in the morning, and found Max tightly wrapped in a blanket with only arm free (see picture at the bottom of this post). I held him for a couple of hours while he snoozed. (We did some arm exercises with the one unswaddled arm.) Before I left I changed his diaper and took his temperature. It's always a rodeo, made somewhat more difficult by the radical incline the NICU team have Max sleeping on. He woke up in the middle of it, and I took the opportunity to do some leg exercises too.
When Carolyn got there Max was back to sleep, but woke up when she picked him up. She took the opportunity to do more exercises. He fell asleep in the middle of a leg lift.
No medical news to report. His breathing seems a little more comfortable, thanks to the combination of ND tube, Lasix, and, maybe, radically tilted bed.

When Carolyn got there Max was back to sleep, but woke up when she picked him up. She took the opportunity to do more exercises. He fell asleep in the middle of a leg lift.
No medical news to report. His breathing seems a little more comfortable, thanks to the combination of ND tube, Lasix, and, maybe, radically tilted bed.
In the step-down NICU
Here's a long shot of Max's new place in the step-down NICU, or "CCN2". The NICU team have Max on a radically slanted bed to help with reflux. He sometimes manages to squirm his way to the bottom of the incline.

Friday, January 2, 2009
Lasix works
Nurse T. (a first-timer with Max---we're always surprised to meet someone new after almost three months in the NICU) reports that Max is having a quiet night. He was awake and alert for his 8:30 PM diaper change but is currently snoozing. The Lasix has continued its work all day and Max has had a series of very heavy diapers and lost 45 grams over the past 24 hours. Nurse T. got Max to suck on a pacifier. His sats remain in the high 90s, suggesting that either the Lasix or the ND tube is in fact giving him some respiratory support. However, Max is still prone to sudden but brief drops in his oxygen saturation. We think he's doing a little better on this front too, though.
Even after losing some weight, Max now weighs in at a hefty 3.3 kilos, or 7 lbs 5 ounces. One of the outfits Carolyn is dressing him has paws for feet. Also, Max now has several frog-themed outfits.
Even after losing some weight, Max now weighs in at a hefty 3.3 kilos, or 7 lbs 5 ounces. One of the outfits Carolyn is dressing him has paws for feet. Also, Max now has several frog-themed outfits.
Original due date
Today marks both Max's 10 week anniversary in the NICU and Max and Ada's original due date. In one sense, Max is now a full term baby (and at about 7 pounds he certainly weighs as much as many terms babies). In reality, though, as nice as the NICU is, a day in the NICU can't compare with a day in the womb.
Max seems to have his days and nights swapped around, so that last night--when Carolyn and I were at home--he was quite active but today--with Carolyn there all day--he was quite drowsy. Needless to say, we'd prefer Max to be the same wake/sleep schedule as the rest of the world (college students excepted). Because Max is more active at night than during the day, the nurses are getting to know him a little better than we do. They report that he likes to be picked up to be soothed.
In medical news, Max gained more than 100 grams overnight but his diapers were relatively light, suggesting that he's retaining fluids. This can contribute to difficulty breathing, so the NICU team put Max on Lasix.
Carolyn tried exercising Max and getting him to use a pacifier. In both cases he seemed more interested in sleeping than in exercising.
Carolyn did learn an interesting fact about Max's condition and the NICU team's plan for him from physical therapist S. She said that (I'm paraphrasing) when it comes to the suck-swallow motion, Max's form, his technique, is fine. However, his endurance is poor. It takes Max a lot of effort to suck or swallow, so that he quickly becomes exhausted. Why is this? Because Max is devoting a large amount of effort to simply breathing. The plan is to let Max's lung capacity develop by feeding him with an ND tube, which ought to cut down on food aspiration. S. said that all babies learn to suck and swallow; the most urgent job for Max now is to get strong.
Max seems to have his days and nights swapped around, so that last night--when Carolyn and I were at home--he was quite active but today--with Carolyn there all day--he was quite drowsy. Needless to say, we'd prefer Max to be the same wake/sleep schedule as the rest of the world (college students excepted). Because Max is more active at night than during the day, the nurses are getting to know him a little better than we do. They report that he likes to be picked up to be soothed.
In medical news, Max gained more than 100 grams overnight but his diapers were relatively light, suggesting that he's retaining fluids. This can contribute to difficulty breathing, so the NICU team put Max on Lasix.
Carolyn tried exercising Max and getting him to use a pacifier. In both cases he seemed more interested in sleeping than in exercising.
Carolyn did learn an interesting fact about Max's condition and the NICU team's plan for him from physical therapist S. She said that (I'm paraphrasing) when it comes to the suck-swallow motion, Max's form, his technique, is fine. However, his endurance is poor. It takes Max a lot of effort to suck or swallow, so that he quickly becomes exhausted. Why is this? Because Max is devoting a large amount of effort to simply breathing. The plan is to let Max's lung capacity develop by feeding him with an ND tube, which ought to cut down on food aspiration. S. said that all babies learn to suck and swallow; the most urgent job for Max now is to get strong.
Thursday, January 1, 2009
ND tubes mean continuous feeding
Carolyn just phoned the NICU and got the nightly update on Max. She also reminded me that, with his new ND tube, Max is not fed every three hours as he had been. Instead, he gets a continuous trickle (20 ccs/hour) because the the duodenum cannot handle large quantities at a time. Max's food now hangs on what looks like an IV bag.
Max's night nurse, J., has had him for three nights now. She felt that his breathing was perhaps a little easier (he was "retracting" -- a sign of respiratory distress -- less often). She also thought that his head felt better, i.e. the fontanel was softer. As always we update his head circumference every night. Over the past few nights, Max's cranial growth rate has run just a little faster than the 0.5 cm/week rate that it had averaged since late November. No one seems to be concerned about this.
Finally, Carolyn informs me that Max has outgrown a lot of his preemie outfits and is now being dressed in normal newborn clothes. Can it be long before the "statistically significant" onesie reappears?
Max's night nurse, J., has had him for three nights now. She felt that his breathing was perhaps a little easier (he was "retracting" -- a sign of respiratory distress -- less often). She also thought that his head felt better, i.e. the fontanel was softer. As always we update his head circumference every night. Over the past few nights, Max's cranial growth rate has run just a little faster than the 0.5 cm/week rate that it had averaged since late November. No one seems to be concerned about this.
Finally, Carolyn informs me that Max has outgrown a lot of his preemie outfits and is now being dressed in normal newborn clothes. Can it be long before the "statistically significant" onesie reappears?
First day on an ND tube
Like lots of people all over the world, Max spent last night throwing up. However, unless there's been a sudden increase in the popularity of barium-based cocktails, I think Max was vomiting for a completely different reason than, say, the college kids who live next door to us. Max's swallowing study yesterday required him to drink some barium-laced milk, which can cause stomach upset. I think he settled down starting with him 8:30 AM feeding.
Max also got a different kind of feeding tube installed today. The NICU put in what I believe is called an "ND", or nasal-duodenal, tube (as opposed to the previous "NG", or nasal-gastric, tube). If I have this right, the tube passes through the pylorus and delivers food to duodenum. The idea is that this reduce Max's habit of inhaling the contents of his stomach that pass up the esophagus because of his reflux. The NICU team think that this "reflux aspiration" is affecting his lungs. They hope that the ND tube will lessen the reflux and give his lungs a chance to develop.
In the spirit of the season, a picture from one year ago today (we've got to quit spending the holidays in hospitals):

Max also got a different kind of feeding tube installed today. The NICU put in what I believe is called an "ND", or nasal-duodenal, tube (as opposed to the previous "NG", or nasal-gastric, tube). If I have this right, the tube passes through the pylorus and delivers food to duodenum. The idea is that this reduce Max's habit of inhaling the contents of his stomach that pass up the esophagus because of his reflux. The NICU team think that this "reflux aspiration" is affecting his lungs. They hope that the ND tube will lessen the reflux and give his lungs a chance to develop.
In the spirit of the season, a picture from one year ago today (we've got to quit spending the holidays in hospitals):
Subscribe to:
Posts (Atom)




