It is an understatement to say that, for much of the past year, Max's medical management and feeding issues have dominated our daily (and nightly) interactions with him. But it feels like we are getting to the point where those things, while still constant, are far from the defining features of life with Max.
Especially thinking back to a year ago, Max has come so far: It was the Tuesday after Thanksgiving that Andreas and I met with the neurosurgeon at Children's to get a second opinion on strategies being used by the Georgetown NICU docs to manage Max's intracranial pressure. (It still amazes me that this neurosurgeon responded to our email on the day after Thanksgiving, called us, and arranged to see us the following Tuesday. He is amazing doc, and one we are willing to wait 3 hours to see -- see story below). Max got his last lumbar tap on Thanksgiving day last year; he was still having breathing problems with regular desats, apnea episodes, and heart rate fluctuations; and his reflux would not be evident until a month from now. It is truly amazing how far Max has come. He is one tough kid.
Of course Max's days of medical management, feeding challenges, and therapies continue. Here's an update on his various fronts:
*
Hydrocephalus. Max had a CT scan and saw the neurosurgeon Dr. K on Nov. 16. We were at Children's Hospital from 9 am until 2 pm. Long day, but Max handled it like a champ (sleeping for 1.5 hours on my shoulder). The CT showed that his ventricles are stable but still "generous" in Dr. K's words. Max's head is growing and still much larger than kids his age, but his growth in on his own concave trajectory which is expected. Max was throwing the ball around the exam room while Dr. K ran after it. A good time was had by all, and Dr. K said that he would not recommend putting in a shunt at this point. We return to Dr. K in 6 months for another CT and checkup (or before if any signs of pressure appear).
*
NG Tube / feeding / weight gain. Max is still fed through the NG tube while he sleeps at night. During the day, he eats pureed food by spoon, little puffs (which he is learning to pick up with his fingers), and formula from the bottle. At a single "meal," he might eat just 1/3 to 1/2 of a jar of baby food, but he does so willingly and we just stop when he turns away. His oral intake of formula from the bottle is anywhere from 200-350 cc per day. His reflux seems to be gone or very well under control, though every once in a while he does have emesis. We think this is from choking on his tube, but maybe the reflux is still a factor. But for now at least, it looks like Max will avoid the fundoplication surgery (where the stomach is tied around the esophagus to stop the reflux).
So Max has shown that he CAN eat by mouth. Why does he still have the NG tube? Well, he's had it for over a year now and his body has become accustomed to it. Why eat by mouth when you can have it delivered directly? We can't just pull it out and let him go hungry for long periods of time because of his nutritional needs for physical and cognitive growth (the GI doc says that studies show it takes monkeys about 2 weeks to develop a normal hunger-eating cycle).
The GI team has given us a plan to wean Max very slowly from the NG tube. If this works, he can avoid getting a stomach tube (G-tube) for feeding. If the process stalls and it looks like the NG tube needs to come out for breathing or speech purposes, then at some point Max may still need a G-tube.
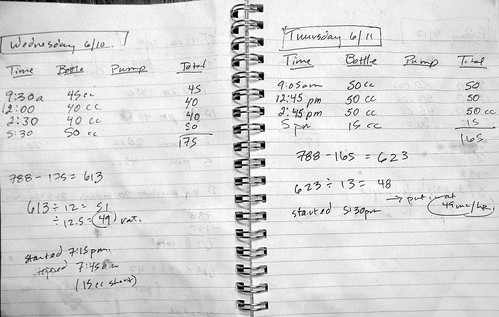
Here's the plan: Max gets weighed every 2 weeks, and if he gains 5 ounces, then we cut back 2 ounces from his nighttime tube feedings. The hope is that he will slowly pick up the slack during the day. We rented a home scale so we can always measure him on the same scale and don't have to take him to a doctor's office just to get weighed. So far, over about a month, Max gained 13 ounces in the first 2 weeks; then 5 ounces in the second 2 weeks. That makes his current nighttime volume through the NG tube 360 cc (or about 12 ounces).
And for the record, Max now weighs 19 lbs 8 ounces, and is 29 inches long.
*
Sleeping. Because Max still gets fed through the NG tube at night, he still has to sleep in his crib, on a 30 degree incline, on his stomach, in the
Tucker sling while the feed is running. He typically wakes up around 4 or 5 a.m. and wants to move around, but can't because he's strapped in the sling. Because his feed is now ending around 3:30 or 4 a.m., he doesn't need to be in the sling all night. So when he wakes up, we move him to his Pack & Play to sleep for the rest of the night. He seems to like this because he can move around and get comfortable. Instead of waking up for the day at 6 am, he is now sleeping until 7 or even 8 am! This is good, because if he really wants to be part of our family, he CANNOT be an early riser.
*
Medicines. Max is now on 4 medicines, delivered at 4 humane times of the day (7 a.m., 3 p.m., bedtime, and 11 p.m.). We recently changed dosages and timing to eliminate the 2 a.m. medicine. Andreas is very happy! Current meds are: Prevacid (for reflux); Erythromycin (an antibiotic which at low doses is used for motility); Culturelle (a probiotic that keeps good bacteria in his stomach); and a multivitamin with iron. As of late September, the pulmonary docs said Max did not need his diuretic (Aldactazide) any more.
*
Therapies. Max is getting speech therapy (for eating) once every 3 weeks, physical therapy once every 2 weeks, and occupational therapy once every 1-2 weeks. And of course Doris therapy every weekday.
*
Vaccines. Max was on top of the list for the H1N1 vaccine. In fact, we all got a dose back in early October when the vaccines were first available, thanks to Max's high-risk status. At his 1-year physical a few days ago, Max got his second dose of the H1N1 vaccine, his second dose of the seasonal flu vaccine, and his vaccines for DTaP, polio, and something else. I thought we might be in for a miserable weekend, but he seems to have shaken all those vaccines off. Let's keep our fingers crossed.
*
Synagis. Max was also approved by our insurance company for a cycle of
Synagis this year. It is a monthly shot of antibodies, delivered October through April, to protect against respiratory syncytial virus (RSV). Each shot is pretty expensive, and we are relieved that our insurance is covering this.
That's it for the medical roundup. Keep watching for other more exciting Max updates.
















































{kind=link}
{kind=link}
{kind=link}