PT with Max from Codered Summer on Vimeo.
Sunday, May 31, 2009
Play is physical therapy
In this video, Carolyn puts Max through his paces: rolling over, stretching and some tummy time, all the while convincing him that it's part of a game. Max, like all children and first-time actors, can't stop from staring at the camera. When I'm not filming him, he focuses a lot more on Carolyn and smiles even more.
Max's Tricks
This five-minute video shows Max doing some of his tricks. Max is watching us eat dinner (including Felix encountering seaweed salad for the first time) and chewing on his blanket, perhaps out of sympathy. We've got the tray latched on to his kidcart; it makes a convenient place to store toys.
You can hear Carolyn and me discussing the fate of a bowl of Felix's cereal, where we resort to spelling out key words. I got H-A-L-F-W-A-Y through a bowl before I decided it was D-I-S-G-U-S-T-I-N-G.
Max's Tricks from Codered Summer on Vimeo.
Saturday, May 30, 2009
Cheers!
A strange meteorological phenomenon is gripping the Washington area--newscasters agree that the weather is no longer trying to kill an unprotected human. We took advantage of the weather to enjoy dinner on our back deck. For the unfamiliar, the "deck" is a rude wooden platform cantilevered off the side of the house; it is mainly used to repel pirates, but does just fine as an informal seating area.
In the picture, I am toasting Max. I am enjoying a snippy sauvignon blanc from Trader Joe's; Max is enjoying an excellent fortified MBM.

In the picture, I am toasting Max. I am enjoying a snippy sauvignon blanc from Trader Joe's; Max is enjoying an excellent fortified MBM.
Friday, May 29, 2009
Carry-out PT
Carolyn and I are getting Max a la carte physical therapy sessions; although he has a pretty settled routine of speech and occupational therapy, we are still looking for an available physical therapist. Until now, all the therapists have come to our house. Today, Carolyn took Max to a therapy center, a sort of carry-out PT. It wasn't such a big hit with either mother or son. We'll see what else is on the menu next week.
Max's fontanel has really felt quite full to us over the past few days. This past Tuesday, Dr. J. found that his head circumference had increased 0.75 inches in the previous week. Taken together, the evidence suggests that Max isn't pulling off the incredible last-minute change in his body chemistry he would need to avoid a shunt. Our next appoint with the Children's phrenology service is a week from Monday. The long drama of Max's flirtation with hydrocephalus is probably drawing to a close, while an exciting new book on managing an indwelling shunt is about to begin.
I knocked off work early today and got home in time to give Max his bath and put him to bed. After a week of only seeing him during the night shift, I was struck again by how fundamentally happy he is. He seems to find the world a source of endless delight. I tried to get a picture of him flashing his trademark gaping grin or his delighted laugh, but like many children he gets very solemn when the camera comes out.
Instead, I took a picture of Max on his wedge trying to get to sleep. This is the one part of the day where he's really quite unhappy. It's the start of the night shift, I suppose. Max "swims" on his wedge, churning his arms and legs around, while Carolyn or I try to soothe him. He eventually settles down and sleeps quite deeply for the first part of the night.
Here is a picture of Max swimming on his wedge:

Max's fontanel has really felt quite full to us over the past few days. This past Tuesday, Dr. J. found that his head circumference had increased 0.75 inches in the previous week. Taken together, the evidence suggests that Max isn't pulling off the incredible last-minute change in his body chemistry he would need to avoid a shunt. Our next appoint with the Children's phrenology service is a week from Monday. The long drama of Max's flirtation with hydrocephalus is probably drawing to a close, while an exciting new book on managing an indwelling shunt is about to begin.
I knocked off work early today and got home in time to give Max his bath and put him to bed. After a week of only seeing him during the night shift, I was struck again by how fundamentally happy he is. He seems to find the world a source of endless delight. I tried to get a picture of him flashing his trademark gaping grin or his delighted laugh, but like many children he gets very solemn when the camera comes out.
Instead, I took a picture of Max on his wedge trying to get to sleep. This is the one part of the day where he's really quite unhappy. It's the start of the night shift, I suppose. Max "swims" on his wedge, churning his arms and legs around, while Carolyn or I try to soothe him. He eventually settles down and sleeps quite deeply for the first part of the night.
Here is a picture of Max swimming on his wedge:
Wednesday, May 27, 2009
Job posting
Wanted: High-energy, goal-driven achiever to support a young, high-growth entrepreneurial enterprise. Duties include scheduling visits by, and managing the egos of, multiple medical professionals, negotiating and manipulating interlocking bureaucracies, planning, executing and tracking complex financial transactions, and operating light machinery. Must be able to divide accurately by 43.
Max could really use a professional manager to schedule and track all of his appointments, therapists, medical records, hospital visits, insurance forms and so forth. For now, he'll have to make do with just us and our total inability to divide accurately by 43.
I'm thinking of Max's schedule because we finally had a physical therapist come to visit. The HSC team had suggested that Max receive physical therapy twice weekly. The available physical therapists in Arlington are so overwhelmed with other patients that this was the first possible appointment, and we will not be seeing this therapist again.
That said, Max had a great time, and Carolyn felt that she learned a lot of new techniques from the therapist. The therapist noted that Max's cognitive awareness and ability have outstripped his physical frailties. He isn't able to reach for the toy, but he clearly wants the toy, and this is a good sign.
Among the toys that Max really likes are, of course, his feet. The therapist at one point brought Max's feet up near his face. He reached out and grabbed them, the first time he's done so.
Tuesday, May 26, 2009
The biggest loser
One the last TV shows that Carolyn and I watched before our forcible removal from popular culture was a reality TV program called The Biggest Loser; obese people competed to lose weight, resist temptation and, this being reality TV, plot to destroy each other. The dramatic moments centered around the weigh-ins, where the week's biggest loser would be revealed. At the time, Carolyn and I speculated about emergency weight loss strategies that a contestant might use to drop the final few ounces before the weigh-in.
We're watching Max's weight with the same intensity that the audience watched those long-ago contestants' weights. In the way that everything in our life is a mirror image of reality as we used to know it, we are desperate to see Max gain weight, and we would be willing to use a trick or two to artificially inflate his weight around his weigh-ins, but the nurses and doctors know about the obvious strategies.
When travelling nurse J. came by on Friday, she found Max to weigh 15 lbs, 1 oz. Dr. J. felt that this was insufficient gain over the week, and asked to see Max after the weekend, i.e. today. Carolyn brought Max in to the pediatrician's office, where they found his weight to be 15 lbs, 5 oz. To me, it's a simple matter of measurement error: different scales, different people doing the weighing, and our floors aren't exactly level. But it seemed to satisfy Dr. J., who asked what we had done over the weekend to increase his weight 1.6 percent in three days.
I'll let you in our secret: we forgot to feed him. At some point last night, probably around 2 or so, his pump ran dry. Carolyn and I slept through our alarms and didn't get up to refill his pump until past 4:00 AM. Just think how much Max would have weighed if we had remembered to feed him.
We're watching Max's weight with the same intensity that the audience watched those long-ago contestants' weights. In the way that everything in our life is a mirror image of reality as we used to know it, we are desperate to see Max gain weight, and we would be willing to use a trick or two to artificially inflate his weight around his weigh-ins, but the nurses and doctors know about the obvious strategies.
When travelling nurse J. came by on Friday, she found Max to weigh 15 lbs, 1 oz. Dr. J. felt that this was insufficient gain over the week, and asked to see Max after the weekend, i.e. today. Carolyn brought Max in to the pediatrician's office, where they found his weight to be 15 lbs, 5 oz. To me, it's a simple matter of measurement error: different scales, different people doing the weighing, and our floors aren't exactly level. But it seemed to satisfy Dr. J., who asked what we had done over the weekend to increase his weight 1.6 percent in three days.
I'll let you in our secret: we forgot to feed him. At some point last night, probably around 2 or so, his pump ran dry. Carolyn and I slept through our alarms and didn't get up to refill his pump until past 4:00 AM. Just think how much Max would have weighed if we had remembered to feed him.
Monday, May 25, 2009
At the chalk party
At the chalk party
Originally uploaded by andreas.lehnert
Breakfast scene
This is a common breakfast scene. Felix is getting some cereal while Max looks on. In this case, Max is in his kidcart; he's often in his bouncy seat. The kidcart has a tray that allows him to play with toys and has other benefits. I have my reservations about the kidcart, but that's a discussion for another day. If nothing else, the kidcart lets Max have a better view of that which he is most fascinated by: his older brother.

Sunday, May 24, 2009
In the bouncy seat, on the deck
In the bouncy seat, on the deck
Originally uploaded by andreas.lehnert
The night shift
I've been taking the night shift this weekend; Carolyn spends the night in the basement while I remain upstairs to keep the home hospital going through the night. In case of emergency I have Carolyn's cell phone number; because the basement is so quiet and isolated from the rest of the house, the telephone really is the only practical way to communicate. So far I haven't broken down and called for help, but it is a three-day weekend.
The night shift at our house poses some unexpected challenges. While I've always had a vague impression of lots of nighttime activity, I haven't had to really grapple with it until now. There's a great deal of arithmetic. Really hard arithmetic.
Here's an example of the kind of story problem I found myself solving last night. Max's pump delivers food at the rate of 43 ccs/hours. He is supposed to get a total dose of 588 ccs and the feed started at 7:30 PM. I was supposed to wake up at 2:00 PM to give him some meds and top up the bag. It's now 4:10 AM and the bag is empty. The pump says that it's delivered 430 ccs. I have a vague sense that it ran out of food around 3:00 AM and has been pumping in air since then. How much more do I need to program the pump to deliver? What about those meds Max was supposed to get at 2:00 AM? Will I remember to delay his next dose two hours so he doesn't get two too close together? Just how guilty should I feel for inflating my son like a basketball? Why didn't I wake up at 2:00?
In short, there's a great deal of division by 43, which is not a natural unit at all. Not to mention fiddling around with the pump in Max's room, which is usually bright and charming, but which is made tenebrous by the extremely late hour.
When Max was in the Georgetown NICU, the nurses encouraged us to have "skin-to-skin" time with him. According to the NICU team, skin-to-skin promoted brain growth and bonding; it may have had benefits for the child too, I don't remember. I'd strip to the waist and they'd hand me Max, clad only in a diaper. We'd sit in a rocking chair, Max held to my chest (and, um, ample tummy). The nurses would only let me take Max out for 20 minutes at a time. But even after such a brief period I would feel totally drugged. There's an ancient part of our brains that is wired to soothe and protect a baby; that primitive cave parent brain would hijack my higher functions completely after just a few minutes of skin-to-skin time. Good-bye seminars, traffic and weather together on the 8s, job evaluations, dinner invitations; hello roasted bison and growling at the dark. Now that we're at home, the cave parent is relegated to taking control only during the night shift; he's there to make sure his son gets everything he needs no matter how tired the modern parent is. The only problem is, the cave parent can't divide by 43.
The night shift at our house poses some unexpected challenges. While I've always had a vague impression of lots of nighttime activity, I haven't had to really grapple with it until now. There's a great deal of arithmetic. Really hard arithmetic.
Here's an example of the kind of story problem I found myself solving last night. Max's pump delivers food at the rate of 43 ccs/hours. He is supposed to get a total dose of 588 ccs and the feed started at 7:30 PM. I was supposed to wake up at 2:00 PM to give him some meds and top up the bag. It's now 4:10 AM and the bag is empty. The pump says that it's delivered 430 ccs. I have a vague sense that it ran out of food around 3:00 AM and has been pumping in air since then. How much more do I need to program the pump to deliver? What about those meds Max was supposed to get at 2:00 AM? Will I remember to delay his next dose two hours so he doesn't get two too close together? Just how guilty should I feel for inflating my son like a basketball? Why didn't I wake up at 2:00?
In short, there's a great deal of division by 43, which is not a natural unit at all. Not to mention fiddling around with the pump in Max's room, which is usually bright and charming, but which is made tenebrous by the extremely late hour.
When Max was in the Georgetown NICU, the nurses encouraged us to have "skin-to-skin" time with him. According to the NICU team, skin-to-skin promoted brain growth and bonding; it may have had benefits for the child too, I don't remember. I'd strip to the waist and they'd hand me Max, clad only in a diaper. We'd sit in a rocking chair, Max held to my chest (and, um, ample tummy). The nurses would only let me take Max out for 20 minutes at a time. But even after such a brief period I would feel totally drugged. There's an ancient part of our brains that is wired to soothe and protect a baby; that primitive cave parent brain would hijack my higher functions completely after just a few minutes of skin-to-skin time. Good-bye seminars, traffic and weather together on the 8s, job evaluations, dinner invitations; hello roasted bison and growling at the dark. Now that we're at home, the cave parent is relegated to taking control only during the night shift; he's there to make sure his son gets everything he needs no matter how tired the modern parent is. The only problem is, the cave parent can't divide by 43.
Saturday, May 23, 2009
Breakfast on the deck
One of the many winter storms that hit Washington this year smashed up the table we had on our deck. This morning the replacement table arrived, and we wasted no time in enjoying both the table and the warmer weather, which also arrived this morning. (Last week there was "patchy frost", not to mention "bitter cursing".)
Felix insisted on bringing out the school bus to have breakfast too:

Max started off playing with his star, but he was also (as usual) fascinated by his older brother. This isn't quite yet a mutual admiration society, but so far open hostilities haven't broken out. Carolyn and I are planning a series of confidence-building measures. Here's Max holding his toy star:

Breakfast was interrupted by a roaring sound. Was it a neighbor doing some construction? An airplane? Felix correctly identified the sound as a helicopter:

Close examination revealed it to be a "white top", part of the presidential fleet. They often circle Arlington on Saturday mornings, presumably for exercise.

Then it was time for Max to get his breakfast:

It's important to take time out during feeding sessions to play. Important to me, that is; I'm not sure whether this is approved procedure. Max enjoys playing the "hand game", where I help him clap his hands.

Then we tried Max in a couple of other positions:

In the end, Max managed just a few sips from the bottle, despite gumming enthusiastically at it. We blame the bottle's slow-flow nipple; at the noon feeding we'll try a turbo nipple for a change. It is true that our friend D. ("the baby whisperer") is able to get Max to take the entire bottle without resorting to high-throughput nipple technology, but it's possible she doesn't have to contend with the same distractions that we do:

Felix insisted on bringing out the school bus to have breakfast too:
Max started off playing with his star, but he was also (as usual) fascinated by his older brother. This isn't quite yet a mutual admiration society, but so far open hostilities haven't broken out. Carolyn and I are planning a series of confidence-building measures. Here's Max holding his toy star:
Breakfast was interrupted by a roaring sound. Was it a neighbor doing some construction? An airplane? Felix correctly identified the sound as a helicopter:
Close examination revealed it to be a "white top", part of the presidential fleet. They often circle Arlington on Saturday mornings, presumably for exercise.
Then it was time for Max to get his breakfast:
It's important to take time out during feeding sessions to play. Important to me, that is; I'm not sure whether this is approved procedure. Max enjoys playing the "hand game", where I help him clap his hands.
Then we tried Max in a couple of other positions:
In the end, Max managed just a few sips from the bottle, despite gumming enthusiastically at it. We blame the bottle's slow-flow nipple; at the noon feeding we'll try a turbo nipple for a change. It is true that our friend D. ("the baby whisperer") is able to get Max to take the entire bottle without resorting to high-throughput nipple technology, but it's possible she doesn't have to contend with the same distractions that we do:
Friday, May 22, 2009
Max in action
Our friend D. ("the baby whisperer") took a video of Max today. She said that it was the kind of thing that if she had just told us about it, we wouldn't have believed it. And she's right: the video shows Max holding his bottle and drinking from it. Of course, he doesn't hold it particularly well (the video shows D. helping him pick it up after he drops it), and he doesn't get a lot down. But I'm not going to cavil at his performance.
You can also see that Max is delighted by his feet and that he likes to look at people--in this case, he's looking at D., who is taking the video. Oh yes, and you can see that Max likes his feet so much he likes to spend time with his legs sticking out so he can keep an eye on his favorite toys.
You can also see that Max is delighted by his feet and that he likes to look at people--in this case, he's looking at D., who is taking the video. Oh yes, and you can see that Max likes his feet so much he likes to spend time with his legs sticking out so he can keep an eye on his favorite toys.
Max in action from Codered Summer on Vimeo.
Monday, May 18, 2009
A visit to the GI service
Carolyn took Max to Children's for an appointment with the GI service. Because Max's big two challenges are his problems feeding by mouth and his habit of throwing up a lot, we expect the GI service to be a big part of Max's care. Carolyn's experience today was a little disconcerting. She went into the meeting expecting the GI service to identify Max's underlying problem, or at least to lay out a plan for figuring out what the problem is, and then to recommend a course of action to solve the problem. I often fantasize that I'm the CEO of a major company, say MaxCo Inc ("Increasing Your Dry Cleaning Bills Since 2008"), and that the medical and surgical services are my staff. I walk in to the boardroom every morning and demand a rundown on the plan to bring MaxCo to profitability by 2010Q1, like I promised the shareholders. Reality and fantasy didn't diverge much when we were all at the hospital, which had a rigid hierarchy and a clear goal. (And, in truth, given the tab that the real-world Max is running up, he may be generating more revenue than many small businesses these days.)
But we're home now, and I'm cast in the role of a small scale entrepreneur; say, a solar-energy enthusiast or a mortgage broker. No big corporate planning department is going to lay out the three milestones to profitability with appropriate workstreams and interim goals. It's just Carolyn and me trying to piece the puzzle together.
Children's GI service really brought this home. No-one knows, really, why Max is vomiting so much, or why his bottle feeding attempts are trailing off so badly. Moreover, the information Carolyn got from the GI service contradicted information we got from the speech and occupational therapists we've seen. As we expected, the GI service tried to "blame the head", i.e. point to his neurological deficits as the cause of his problems. But beyond that, they didn't have a particular diagnosis, or even really a plan for narrowing down the cause of his problems.
They thought that, perhaps, Max might be getting too much food, as evidenced by the fact that he's gaining weight at the upper end of the normal range. One possibility, they suggested, was to feed him less at night. As an alternative, we could feed him the same amount, but fortify less, so that his food is less rich and hence (I assume) easier to digest. The GI service kept referring to Max's problems as "gagging" as in "perhaps he's gagging on his feeding tube." So they're not even convinced he has reflux. The GI specialists mentioned a type of surgery that we hadn't heard of before: a "peg", which is simple to install and allows access to the stomach through the abdominal wall. Of course, such a device will derange the Angle of His. However, according to the GI specialists, the research on the relationship between stretching the Angle of His from acute to oblique doesn't really support the view that it worsens reflux. Which Max might not have anyway.
In the end, we assembled all of the information and ideas from the GI service and laid them at the feet of Max's pediatrician, the stalwart Dr. J. She called Carolyn back at 9:00 PM tonight and discussed the new information and the options. She agreed that dialing back the fortification was potentially a good step.
Max was absolutely exhausted after his trip up to Children's. He insisted on an early bedtime, and was tucked up and sound asleep by the time I got home from work. I got to go up and give him his 8:00 PM medications, though, and he was extremely cute. Carolyn reports that Max put on his usual display of irresistible charm while at Children's today. However, the hardened professionals of the GI service take a deeply skeptical view of baby charm, perhaps because they are constantly being vomited on by their patients.
But we're home now, and I'm cast in the role of a small scale entrepreneur; say, a solar-energy enthusiast or a mortgage broker. No big corporate planning department is going to lay out the three milestones to profitability with appropriate workstreams and interim goals. It's just Carolyn and me trying to piece the puzzle together.
Children's GI service really brought this home. No-one knows, really, why Max is vomiting so much, or why his bottle feeding attempts are trailing off so badly. Moreover, the information Carolyn got from the GI service contradicted information we got from the speech and occupational therapists we've seen. As we expected, the GI service tried to "blame the head", i.e. point to his neurological deficits as the cause of his problems. But beyond that, they didn't have a particular diagnosis, or even really a plan for narrowing down the cause of his problems.
They thought that, perhaps, Max might be getting too much food, as evidenced by the fact that he's gaining weight at the upper end of the normal range. One possibility, they suggested, was to feed him less at night. As an alternative, we could feed him the same amount, but fortify less, so that his food is less rich and hence (I assume) easier to digest. The GI service kept referring to Max's problems as "gagging" as in "perhaps he's gagging on his feeding tube." So they're not even convinced he has reflux. The GI specialists mentioned a type of surgery that we hadn't heard of before: a "peg", which is simple to install and allows access to the stomach through the abdominal wall. Of course, such a device will derange the Angle of His. However, according to the GI specialists, the research on the relationship between stretching the Angle of His from acute to oblique doesn't really support the view that it worsens reflux. Which Max might not have anyway.
In the end, we assembled all of the information and ideas from the GI service and laid them at the feet of Max's pediatrician, the stalwart Dr. J. She called Carolyn back at 9:00 PM tonight and discussed the new information and the options. She agreed that dialing back the fortification was potentially a good step.
Max was absolutely exhausted after his trip up to Children's. He insisted on an early bedtime, and was tucked up and sound asleep by the time I got home from work. I got to go up and give him his 8:00 PM medications, though, and he was extremely cute. Carolyn reports that Max put on his usual display of irresistible charm while at Children's today. However, the hardened professionals of the GI service take a deeply skeptical view of baby charm, perhaps because they are constantly being vomited on by their patients.
Sunday, May 17, 2009
Tube free (for a little while)
Max pulled out his ng tube this morning, giving me an opportunity to take plenty of tube-free pictures. Of course, we immediately worked to reinsert the tube, so Max didn't get to enjoy his freedom for very long. Max had kept this tube in about two weeks, so we switched nostrils.
Max won't be rid of the tube for good until he starts taking a significant amount of food by mouth. He gets about 700 ccs of milk or formula per day. Today, he managed to get down 19 ccs by mouth, although we were quite happy because this is a lot more than he usually takes over a weekend.

Max won't be rid of the tube for good until he starts taking a significant amount of food by mouth. He gets about 700 ccs of milk or formula per day. Today, he managed to get down 19 ccs by mouth, although we were quite happy because this is a lot more than he usually takes over a weekend.
Saturday, May 16, 2009
Occupational therapy for babies
Occupational therapist C. visited Max today; this is only the second therapeutic visit Max has had since coming home. Carolyn is slowly figuring out the bureaucratic maze surrounding service providers. It's particularly troubling that Max has yet to see a speech therapist, given that his primary problem right now is eating by mouth.
C. specializes in baby massage. Maybe I was skeptical; now, I'm a believer. C. used something like a beneficent version of the Vulcan nerve pinch on Max. A couple of simple strokes and suddenly Max is smiling and gurgling happily.
C. also watched Carolyn give Max a bottle. It was shaping up to be another dud session, but C. applied very slight pressure to Max's temples and cheeks and he eagerly gulped down most of the bottle. He did so well, in fact, that his stomach rebelled and he vomited back about half of the feed. But no matter!
I wonder if perhaps Max's new friends can have great success feeding him at first, before he begins to associate them with food. Max long ago figured out that when Carolyn or I prop him up in the crook of our arm, we're going to try to feed him. But when these new people (the baby whisperer, C. et al) try, Max is caught off guard and he is anyway too polite to throw a tantrum in front of a stranger. Perhaps the secret to feeding Max will not be, as all the books advise, to put him in a calm familiar place but rather to surprise him with an unexpected bottle in novel surroundings.
C. specializes in baby massage. Maybe I was skeptical; now, I'm a believer. C. used something like a beneficent version of the Vulcan nerve pinch on Max. A couple of simple strokes and suddenly Max is smiling and gurgling happily.
C. also watched Carolyn give Max a bottle. It was shaping up to be another dud session, but C. applied very slight pressure to Max's temples and cheeks and he eagerly gulped down most of the bottle. He did so well, in fact, that his stomach rebelled and he vomited back about half of the feed. But no matter!
I wonder if perhaps Max's new friends can have great success feeding him at first, before he begins to associate them with food. Max long ago figured out that when Carolyn or I prop him up in the crook of our arm, we're going to try to feed him. But when these new people (the baby whisperer, C. et al) try, Max is caught off guard and he is anyway too polite to throw a tantrum in front of a stranger. Perhaps the secret to feeding Max will not be, as all the books advise, to put him in a calm familiar place but rather to surprise him with an unexpected bottle in novel surroundings.
Getting caught in the rain
Now that Max is home, he can experience the full range of sensations offered by life outside of the hospital. And one of those is the feeling of rain pelting down amid impressive thunder and lightening. (Not to mention the sense of speed as his father races the stroller to shelter.) Here, Max and an unknown biker wait out a thunderstorm under a bridge.

Friday, May 15, 2009
How to get a tube-fed baby to take a bottle
Actually, we don't know how to get Max, who has been exclusively fed by an ng tube, to take a bottle routinely. Earlier this week I had a giddy feeling that Max was doing so well with his bottle feedings--thanks to the secrets of the baby whisperer--that he might forgo the pump completely during the day. But as the week wore on, D. ("the baby whisperer") found it harder and harder to get Max to take a bottle. Carolyn had a long conversation with D. regarding oral aversion and feeding problems, the upshot of which was D.'s feeling that she had been pushing Max too hard and probably he was getting grumpy whenever the bottle came into view. We all scaled back our expectations and went back to the standard three PO attempts per day. ("PO" is medical jargon for "by mouth"). So the bad news is that I've had to scale back my vision of Max just bursting out of his cocoon to turn into a butterfly in a month. But the good news is that, with more realistic goals, Max is doing extremely well.
In other news, Max and Carolyn went to visit his pediatrician. The big downer is that the office had lost Max's chart. Experiences like this are what lead reasonable people to conclude that simple efficiency improvements ("like we have at my office") could save $2 trillion per year in medical expenses. But, really, who hasn't lost the chart (or equivalent) at their job from time to time? The main consequence was that, when the pediatricians weighed Max (14 pounds 15 ounces) they didn't know how much weight he had gained.
Otherwise, Max's legs seemed tight and muscular. My theory is that he has figured out how to switch is muscles on and off, but hasn't figured out how to achieve states between tense and relaxed. His range of motion doesn't seem impeded.
While at the peds, Max was, in Carolyn's words, "bright and sparkly". He showed off a new trick: grabbing a stuffed animal resting on his chest while lying on his back. Max did a lot of smiling and was very calm and patient while he was being discussed. When discussing how to watch for signs of personality changes induced by increased intracranial pressure stemming from his hydrocephalus, the pediatrician pointed to a smiling Max and said: "He won't be like that".
In other news, Max and Carolyn went to visit his pediatrician. The big downer is that the office had lost Max's chart. Experiences like this are what lead reasonable people to conclude that simple efficiency improvements ("like we have at my office") could save $2 trillion per year in medical expenses. But, really, who hasn't lost the chart (or equivalent) at their job from time to time? The main consequence was that, when the pediatricians weighed Max (14 pounds 15 ounces) they didn't know how much weight he had gained.
Otherwise, Max's legs seemed tight and muscular. My theory is that he has figured out how to switch is muscles on and off, but hasn't figured out how to achieve states between tense and relaxed. His range of motion doesn't seem impeded.
While at the peds, Max was, in Carolyn's words, "bright and sparkly". He showed off a new trick: grabbing a stuffed animal resting on his chest while lying on his back. Max did a lot of smiling and was very calm and patient while he was being discussed. When discussing how to watch for signs of personality changes induced by increased intracranial pressure stemming from his hydrocephalus, the pediatrician pointed to a smiling Max and said: "He won't be like that".
Monday, May 11, 2009
Secrets of the baby whisperer
Last week I was concerned that Max's run of record-breaking bottle feedings were part of the cycle described by the speech therapists, where babies do well for a few days but then suffer severe reflux pain and eschew the bottle. And we got almost nothing in Max by mouth over the weekend--maybe 20 ccs in total over two days. But the other variable was the absence of our friend D. ("the baby whisperer"). Today D. came back and Max took four bottles, for 35 ccs, 50 ccs, 50 ccs and 25 ccs. I think this marks a new personal best for Max.
Obviously, the reflux cycle isn't at work. Instead, operator error is to blame. Carolyn watched D. give a bottle today and noticed the following secrets to getting a recalcitrant, refluxy, tube-fed baby to take a bottle:
Obviously, the reflux cycle isn't at work. Instead, operator error is to blame. Carolyn watched D. give a bottle today and noticed the following secrets to getting a recalcitrant, refluxy, tube-fed baby to take a bottle:
- Keep it fun! D. sings, tickles and otherwise "gives him input" (e.g. pushing his legs)
- Wrap him up--some babies enjoy being swaddled, and it increases their sense of organization.
- Take plenty of breaks. Max took his feeds at the same (very slow) rate delivered by his pump on average. Getting there, however, he would eat fairly quickly, lose interest, play with toys, and then come back to the bottle.
- Look him in the eye. My crackpot theory is that babies are attuned to faces, and it's comforting to have a big friendly face looming at them.
- "Let him know who's in charge". (Presumably D. meant that she was in charge, but when she's not here, Max totally has us running at his beck and call.
Friday, May 8, 2009
The discreet pleasures of the second act
Last week, everything was new. We had to get the nursery ready (finally)! We had to figure out the pump! The monitor! The medicine schedule! We had our first meetings with the pediatrician and the therapy team. Each of those meetings was really intense, with all of us, including Max, totally focused on figuring out the plan. The room was buzzing with the energy everyone brought, and even Max, who knew he was auditioning for the part of Most Interesting Baby Under My Care, put on major performances at each meeting. Throughout it all, Carolyn and I felt a real sense of progress and direction.
This week, the pump, monitor and medicines are just tools in the home hospital. Carolyn met again with the pediatrician and the therapists, as she will every week for the next couple of months. She reports that everyone was flatter, including Max. For example, Max didn't do very well feeding from his bottle when the therapist was watching, despite having had a string of great days. And it feels like Max's care is a little more aimless, with the team more or less keeping the same regimen. Certainly that initial sense of excitement has dissipated, leaving Carolyn and me to face the quotidian reality of Max's second act.
Actually, although the second acts of most plays can be pretty forgettable, I can sort of see what this is going to be like, and it's going to be good. Max will make incremental progress, with some inevitable setbacks, of course. It's unrealistic to expect a constant stream of dramatic changes like the ones Max has gone through over the past couple of weeks. After all, how often can he come home from the hospital? (Answer: just this one time, I sincerely hope.) And while we won't really notice it, as the months go by, Max will mature and overcome some of his challenges.
Max's second act is off to a good start. I drove home tonight to find Max, Felix and Carolyn in the front yard enjoying a late spring evening. And Max isn't picking up new tricks, but he is improving on his old ones. He is now given to full-on belly laughs. He is absolutely delighted to have his mother tickle his feet.
The trick to this new phase is to actually enjoy each day. The past six months in the hospital were a raw torrent of emotion. Now we have to consider the possibility that we might all, as a family, have actual, drama-free, fun. It's enough to live in this moment, and not to think about what the third act might bring.
This week, the pump, monitor and medicines are just tools in the home hospital. Carolyn met again with the pediatrician and the therapists, as she will every week for the next couple of months. She reports that everyone was flatter, including Max. For example, Max didn't do very well feeding from his bottle when the therapist was watching, despite having had a string of great days. And it feels like Max's care is a little more aimless, with the team more or less keeping the same regimen. Certainly that initial sense of excitement has dissipated, leaving Carolyn and me to face the quotidian reality of Max's second act.
Actually, although the second acts of most plays can be pretty forgettable, I can sort of see what this is going to be like, and it's going to be good. Max will make incremental progress, with some inevitable setbacks, of course. It's unrealistic to expect a constant stream of dramatic changes like the ones Max has gone through over the past couple of weeks. After all, how often can he come home from the hospital? (Answer: just this one time, I sincerely hope.) And while we won't really notice it, as the months go by, Max will mature and overcome some of his challenges.
Max's second act is off to a good start. I drove home tonight to find Max, Felix and Carolyn in the front yard enjoying a late spring evening. And Max isn't picking up new tricks, but he is improving on his old ones. He is now given to full-on belly laughs. He is absolutely delighted to have his mother tickle his feet.
The trick to this new phase is to actually enjoy each day. The past six months in the hospital were a raw torrent of emotion. Now we have to consider the possibility that we might all, as a family, have actual, drama-free, fun. It's enough to live in this moment, and not to think about what the third act might bring.
Wednesday, May 6, 2009
Thriving at home (so far)
One of the first rules of the NICU we learnt was to take it one day at a time--an injunction to discount any day's highs or lows. I suspect there's a similar rule for the home hospital, but Max has had a string of good days. Maybe we're allowed a small measure of confidence and hope, even as we keep an eye on his hydrocephalus and other evolving threats.
Over the past few days Max's ng tube has become sort of disgusting. One of his favorite tricks is vomiting through his nose and messing up the tape holding the tube in place. This morning, Carolyn and D. got sick of it and pulled the tape off and the tube out. Max got to spend most of the day without an ng tube. This meant that he relied solely on the bottle for feeding--no backup recourse to the pump if he couldn't take all his nutrition by mouth. And he did quite well, taking 30 to 40 ccs by bottle at the three regularly scheduled feedings plus one bonus feeding. Of course, each of these feedings takes close to an hour of patient work, but this is great. Although we're thrilled, we keep in mind the warning we got from HSC speech therapist L., who told us to watch for a sinusoidal pattern in Max's bottle feeding. Max might eat a lot to satisfy his hunger, have a bout of reflux and then go off bottle feeds for a while. However, Max hasn't yet had a bad day with the bottle. All of the credit goes to D., who is amazingly patient and has a deep intuitive connection with babies.
I asked Carolyn to take plenty of pictures of Max without his ng tube. She complied. Here's one of my favorites:

Visiting nurse J. came by in the afternoon to supervise the introduction of a fresh tube, along with a cleaner taping job. She brought a new tube style that has a separate port for medicines, so we no longer have to disconnect the pump to give Max his medicines. In addition, the tube stoppers are more robust and easier to manipulate with one hand.
Nurse J. weighed Max, and found that he had gained six ounces since her last visit on Friday. This is a big increase, but Max was probably a little light when she weighed him last, so we think that he's gaining weight at a healthy pace.
As a visiting nurse, I think that part of J.'s job is to gently remind parents of their duties, as well as to help them run the home hospital. J. pointed out that it really was well past time for Max to get a real tub bath. We didn't jump for joy, but we did it (well, D. did). Among other things, a tub bath means that Max's monitor leads have to be taken off and then replaced. Max seemed to enjoy his full immersion, although not quite as much as he enjoys his sponge baths. Here's a picture. Note the tight grip on D.'s finger:

Over the past few days Max's ng tube has become sort of disgusting. One of his favorite tricks is vomiting through his nose and messing up the tape holding the tube in place. This morning, Carolyn and D. got sick of it and pulled the tape off and the tube out. Max got to spend most of the day without an ng tube. This meant that he relied solely on the bottle for feeding--no backup recourse to the pump if he couldn't take all his nutrition by mouth. And he did quite well, taking 30 to 40 ccs by bottle at the three regularly scheduled feedings plus one bonus feeding. Of course, each of these feedings takes close to an hour of patient work, but this is great. Although we're thrilled, we keep in mind the warning we got from HSC speech therapist L., who told us to watch for a sinusoidal pattern in Max's bottle feeding. Max might eat a lot to satisfy his hunger, have a bout of reflux and then go off bottle feeds for a while. However, Max hasn't yet had a bad day with the bottle. All of the credit goes to D., who is amazingly patient and has a deep intuitive connection with babies.
I asked Carolyn to take plenty of pictures of Max without his ng tube. She complied. Here's one of my favorites:
Visiting nurse J. came by in the afternoon to supervise the introduction of a fresh tube, along with a cleaner taping job. She brought a new tube style that has a separate port for medicines, so we no longer have to disconnect the pump to give Max his medicines. In addition, the tube stoppers are more robust and easier to manipulate with one hand.
Nurse J. weighed Max, and found that he had gained six ounces since her last visit on Friday. This is a big increase, but Max was probably a little light when she weighed him last, so we think that he's gaining weight at a healthy pace.
As a visiting nurse, I think that part of J.'s job is to gently remind parents of their duties, as well as to help them run the home hospital. J. pointed out that it really was well past time for Max to get a real tub bath. We didn't jump for joy, but we did it (well, D. did). Among other things, a tub bath means that Max's monitor leads have to be taken off and then replaced. Max seemed to enjoy his full immersion, although not quite as much as he enjoys his sponge baths. Here's a picture. Note the tight grip on D.'s finger:
Monday, May 4, 2009
Another visit to the phrenologists
Carolyn and I took Max to Children's today for another visit with the irrepressible B., the pediatric neurosurgeon who is following Max's hydrocephalus and evaluating him for an indwelling shunt. I took Max to visit B. a month ago. At that visit back in March, B. described Max's ventricles, which are swollen enough to make for a terrifying x-ray, as "generous", thereby earning our undying loyalty. B.'s latest bit of uplift was to describe Max's severely delayed progress as "hitting his milestones at his own pace".
Unfortunately, if Max's ventricles used to be generous back in March, they've since evolved into Mother Theresa. As part of our visit, Max got another CT scan on his skull. B. showed us the most recent results compared with those taken back in March. To the untrained eye, Max's hydrocephalus has gotten markedly worse. To the ever-optimistic B., Max's hydrocephalus had maybe gotten 2 percent worse, or possibly 5 percent, or maybe 10 percent at the very most. His head circumference (which we aren't monitoring daily anymore) has also increased. However, while not yet dangerous (one hopes), at this rate, Max will absolutely need a shunt in the next couple of months. B. has scheduled a follow-up visit for early June. My guess is that if Max's ventricles do anything but become less generous between now and then, B. will schedule Max for surgery. As he was wrapping up, B. gave us his standard line that he was "going to bet on Max".
Perhaps it's simply the exhaustion, but Carolyn and I face the prospect of the coming month's uncertainty regarding Max's shunt with equanimity. In the hospital, we were in a largely passive role: things happened to Max, nothing was under our control. Now that Max is home, we control his feeding schedule, his environment and we make sure he gets sufficient and correct therapy. For the first time in six months, there's a lot of Max's care that we control. Allowing those parts we can't control to play out is somehow easier now.
Here's a picture of Max getting a CT scan of his head:

Unfortunately, if Max's ventricles used to be generous back in March, they've since evolved into Mother Theresa. As part of our visit, Max got another CT scan on his skull. B. showed us the most recent results compared with those taken back in March. To the untrained eye, Max's hydrocephalus has gotten markedly worse. To the ever-optimistic B., Max's hydrocephalus had maybe gotten 2 percent worse, or possibly 5 percent, or maybe 10 percent at the very most. His head circumference (which we aren't monitoring daily anymore) has also increased. However, while not yet dangerous (one hopes), at this rate, Max will absolutely need a shunt in the next couple of months. B. has scheduled a follow-up visit for early June. My guess is that if Max's ventricles do anything but become less generous between now and then, B. will schedule Max for surgery. As he was wrapping up, B. gave us his standard line that he was "going to bet on Max".
Perhaps it's simply the exhaustion, but Carolyn and I face the prospect of the coming month's uncertainty regarding Max's shunt with equanimity. In the hospital, we were in a largely passive role: things happened to Max, nothing was under our control. Now that Max is home, we control his feeding schedule, his environment and we make sure he gets sufficient and correct therapy. For the first time in six months, there's a lot of Max's care that we control. Allowing those parts we can't control to play out is somehow easier now.
Here's a picture of Max getting a CT scan of his head:
Max is babbling a lot more
Max & the rattle
Originally uploaded by andreas.lehnert
Over the past few days, Max has been babbling a lot more. I've been listening for consonants but I can't pick them out of the liquid stream-of-consciousness speaking style Max prefers. I'll leave it to the pediatrician to decide later this week. In the pre-dawn darkness today I tried to capture his logorrhea, but Max broke off his monologue to play with the video camera and the rattle. I'll be on the lookout for my next chance. In the meantime, please enjoy Max being alternatively delighted and frightened by his rattle.
His babbling has an edge of tension to it: if you weren't looking at him, you would think that he was crying, or getting ready to. But he does it all with a big smile on his face, and he usually doesn't break into tears, so he must not be in distress.
On a related note, Max is fascinating by people talking. Carolyn and I were chatting in the kitchen and we noticed his head tracking from speaker to speaker, like at a tennis match. We've seized on this interest to also make a big deal out of eating. "You see, Max, mommy and I are using our mouths ... to eat ... and we've got big smiles on our faces so it must be fun". He doesn't seem ready to give up the tube just yet though.
Saturday, May 2, 2009
The home hospital
Since Max came home Carolyn and I have been operating a small-scale low-intensity care facility from our home. We've become so proficient that we're thinking of running a special needs infant day care center as a way of supplementing our income.
All kidding aside, managing Max's care seemed absolutely overwhelming at first, and, although we've started to settle into a routine, it remains a lot of work. However, it's rewarding work: Max loves getting a sponge bath, for example. In addition, as we gain confidence, we're tweaking Max's care based on our own thinking of what he needs. Of course, our first tentative steps away from the care instructions we came home with resulted in Max losing weight--a big deal for recently released babies. But, seriously, who makes any progress in life without a few missteps? We're learning as we go along.
Because Max can only tolerate a tiny amount of food by mouth, we rely on a pump hooked up to his ng tube to deliver almost all of his calories. If he's going to get over his reflux, he's going to have to get big and strong. Here's a picture of the pump:

The big metal pole is just that: a big metal pole to hang stuff from. The pump is the small box about half-way up. It's an infinity orange model enteral feeding pump. Every morning we break out a new plastic food bag to hang from the metal pole. Max gets formula during the day and fortified breast milk at night. This model pump can handle both formula and the thinner breast milk. The pump has a battery pack that we charge at night and comes with a discreet backpack: we can be extremely mobile, a thrilling though somewhat disorienting prospect.
Max gets a variety of medications delivered through his feeding tube. We use regular syringes:

From the bottom to the top: a probiotic solution, erythromycin (an antibiotic with prokinetic properties) and sterile water to flush the drugs out of the feeding line and into his stomach. Max mainly gets drugs to help control his reflux, although he remains on a small dose of aldactazide (a brand-name combination of diuretics) left over from his lung problems in January. The idea is to let him "grow out" of the dose. The dosage of the other drugs will increase with his weight. Here's a picture of Carolyn delivering medicines (I love the expression on Max's face):

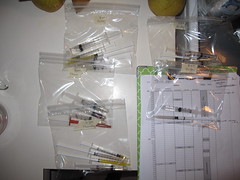
Over the course of the day, Max gets 19 separate doses of drugs, vitamins and so on. We find it easier to make a day's worth of medicines all at once and store them in baggies:
To keep all of this straight, Carolyn put together a daily schedule for Max with his feedings (attempts with the bottle, formula, breast milk etc) and drugs. In addition, we try to record notable events, although the definition of "notable" is becoming a little plastic. Here's a picture of a schedule, sitting next to a recipe for Max's formula:
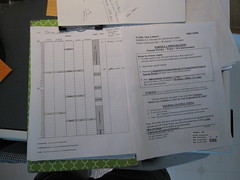
(If you look closely you can see arithmetic in the margins--there's a great deal more long division than I would have thought.)
At night, we hook Max up to his monitor. Thankfully, he left his pulse-ox meter in the hospital, but we do still keep track of his breathing and heart rate. In my opinion, the monitor looks like a Soviet tape-deck, but we're told it's the latest thing in home health care:

The monitor is connected to two leads taped to Max's chest: one measuring his heart rate, and the other measuring his respiration rate. Which is which? You don't want to get them backwards, or the monitor will think that he's taking 170 breaths per minute, but his heart is only 40 beats per minute. There's a handy mnemonic we use: "white on right". Ah-ha, but whose right? (Max's). And who can tell their right from their left in the night? Here is a picture of Max's chest, showing the leads. The leads are sticky, but can't stand up to baby sweat, spit up, etc, so we've added extra tape to hold them in place:

Finally, we keep tabs on Max using a video camera we placed in his room. We had a sound-only pickup in Felix's room that we dubbed "Radio Free Felix". We haven't decided which cable news network the video system best resembles yet.

The monitor has a night-vision feature, showing a grainy black-and-white image in low light. Squinting at the tiny screen always reminds me footage of people watching the Apollo landings back in the 1970s.
All kidding aside, managing Max's care seemed absolutely overwhelming at first, and, although we've started to settle into a routine, it remains a lot of work. However, it's rewarding work: Max loves getting a sponge bath, for example. In addition, as we gain confidence, we're tweaking Max's care based on our own thinking of what he needs. Of course, our first tentative steps away from the care instructions we came home with resulted in Max losing weight--a big deal for recently released babies. But, seriously, who makes any progress in life without a few missteps? We're learning as we go along.
Because Max can only tolerate a tiny amount of food by mouth, we rely on a pump hooked up to his ng tube to deliver almost all of his calories. If he's going to get over his reflux, he's going to have to get big and strong. Here's a picture of the pump:
The big metal pole is just that: a big metal pole to hang stuff from. The pump is the small box about half-way up. It's an infinity orange model enteral feeding pump. Every morning we break out a new plastic food bag to hang from the metal pole. Max gets formula during the day and fortified breast milk at night. This model pump can handle both formula and the thinner breast milk. The pump has a battery pack that we charge at night and comes with a discreet backpack: we can be extremely mobile, a thrilling though somewhat disorienting prospect.
Max gets a variety of medications delivered through his feeding tube. We use regular syringes:
From the bottom to the top: a probiotic solution, erythromycin (an antibiotic with prokinetic properties) and sterile water to flush the drugs out of the feeding line and into his stomach. Max mainly gets drugs to help control his reflux, although he remains on a small dose of aldactazide (a brand-name combination of diuretics) left over from his lung problems in January. The idea is to let him "grow out" of the dose. The dosage of the other drugs will increase with his weight. Here's a picture of Carolyn delivering medicines (I love the expression on Max's face):
Over the course of the day, Max gets 19 separate doses of drugs, vitamins and so on. We find it easier to make a day's worth of medicines all at once and store them in baggies:
To keep all of this straight, Carolyn put together a daily schedule for Max with his feedings (attempts with the bottle, formula, breast milk etc) and drugs. In addition, we try to record notable events, although the definition of "notable" is becoming a little plastic. Here's a picture of a schedule, sitting next to a recipe for Max's formula:
(If you look closely you can see arithmetic in the margins--there's a great deal more long division than I would have thought.)
At night, we hook Max up to his monitor. Thankfully, he left his pulse-ox meter in the hospital, but we do still keep track of his breathing and heart rate. In my opinion, the monitor looks like a Soviet tape-deck, but we're told it's the latest thing in home health care:
The monitor is connected to two leads taped to Max's chest: one measuring his heart rate, and the other measuring his respiration rate. Which is which? You don't want to get them backwards, or the monitor will think that he's taking 170 breaths per minute, but his heart is only 40 beats per minute. There's a handy mnemonic we use: "white on right". Ah-ha, but whose right? (Max's). And who can tell their right from their left in the night? Here is a picture of Max's chest, showing the leads. The leads are sticky, but can't stand up to baby sweat, spit up, etc, so we've added extra tape to hold them in place:
Finally, we keep tabs on Max using a video camera we placed in his room. We had a sound-only pickup in Felix's room that we dubbed "Radio Free Felix". We haven't decided which cable news network the video system best resembles yet.
The monitor has a night-vision feature, showing a grainy black-and-white image in low light. Squinting at the tiny screen always reminds me footage of people watching the Apollo landings back in the 1970s.
Friday, May 1, 2009
Considering a normal family life
This picture shows a scene that would have been difficult to imagine even a week ago. Carolyn, Max, Felix and I are all playing outside. (Max, interestingly, is totally fascinated by his older brother.)
Here, Max is already hooked up to the pump delivering his nightly feeding. However, the pump can be carried in a discreet backpack and operated on battery power, so we're completely mobile.
Carolyn and I are considering the meaning of a normal family life for the first time since she went on bedrest last summer. We're still cautious, but we are considering that the four of us might ... go to a park ... together. I'm still thinking this through.

Here, Max is already hooked up to the pump delivering his nightly feeding. However, the pump can be carried in a discreet backpack and operated on battery power, so we're completely mobile.
Carolyn and I are considering the meaning of a normal family life for the first time since she went on bedrest last summer. We're still cautious, but we are considering that the four of us might ... go to a park ... together. I'm still thinking this through.
Subscribe to:
Posts (Atom)





{kind=link}